

Descemet Stripping Automated Endothelial Keratoplasty (DSAEK)
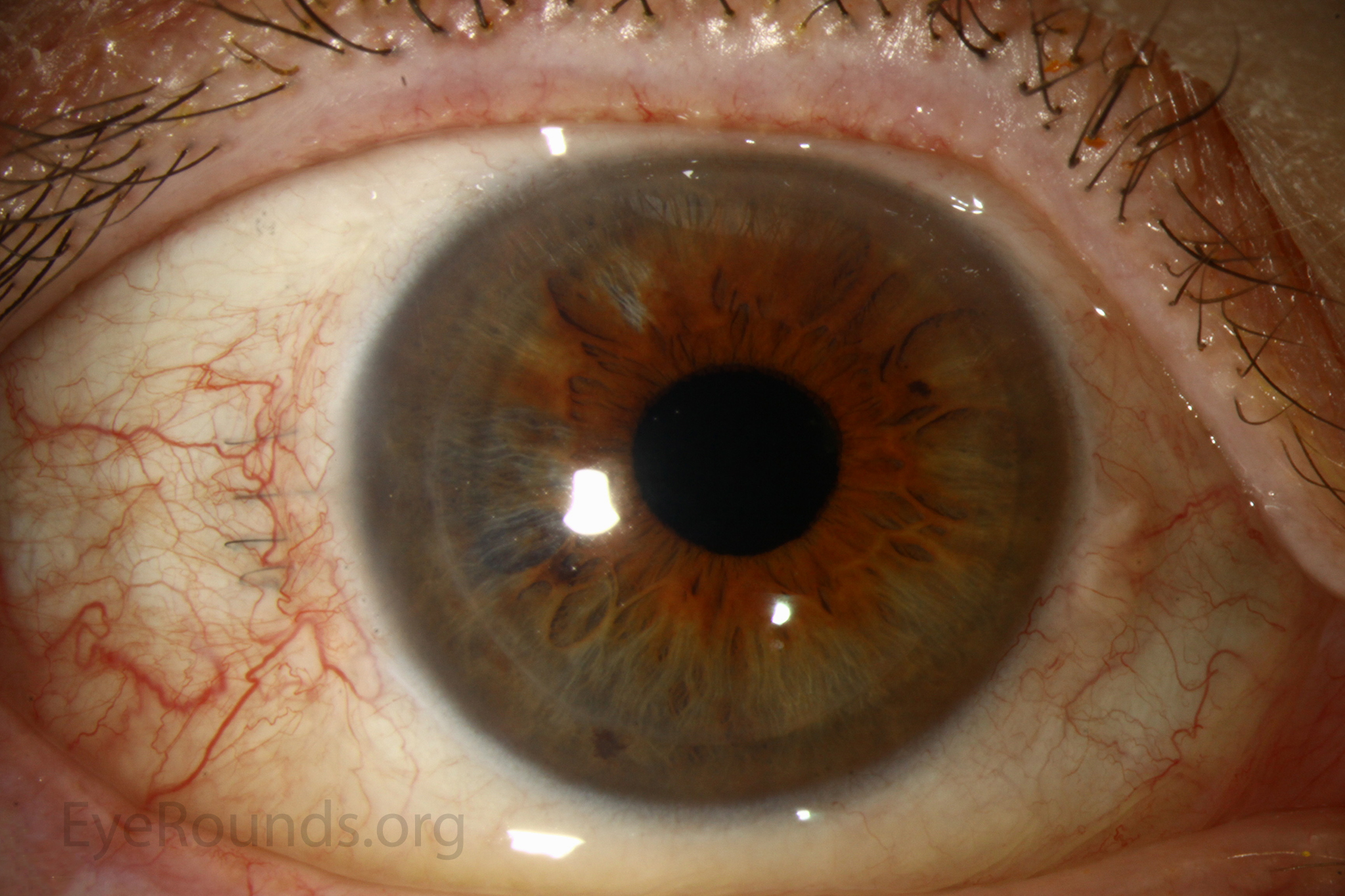
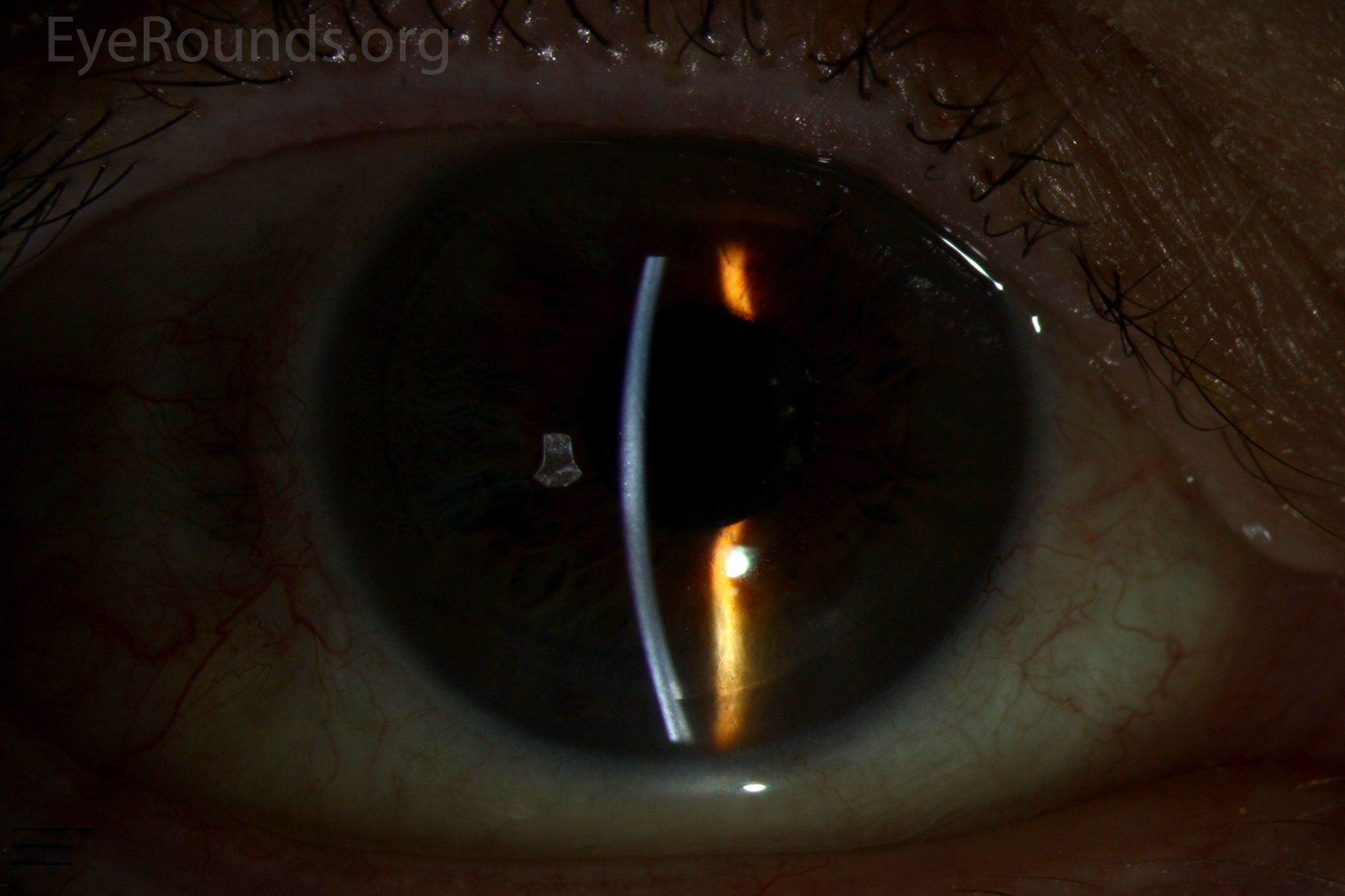
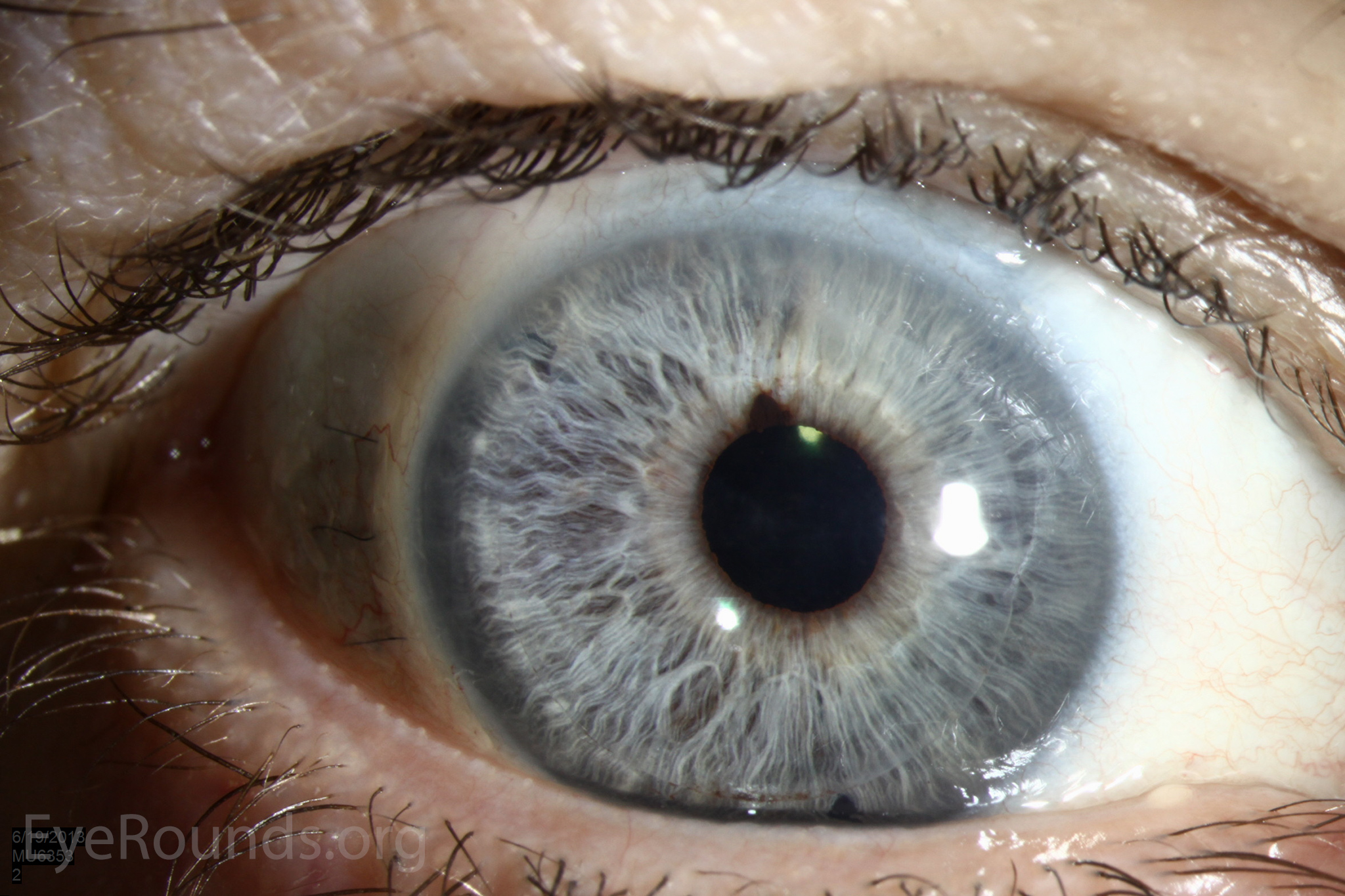
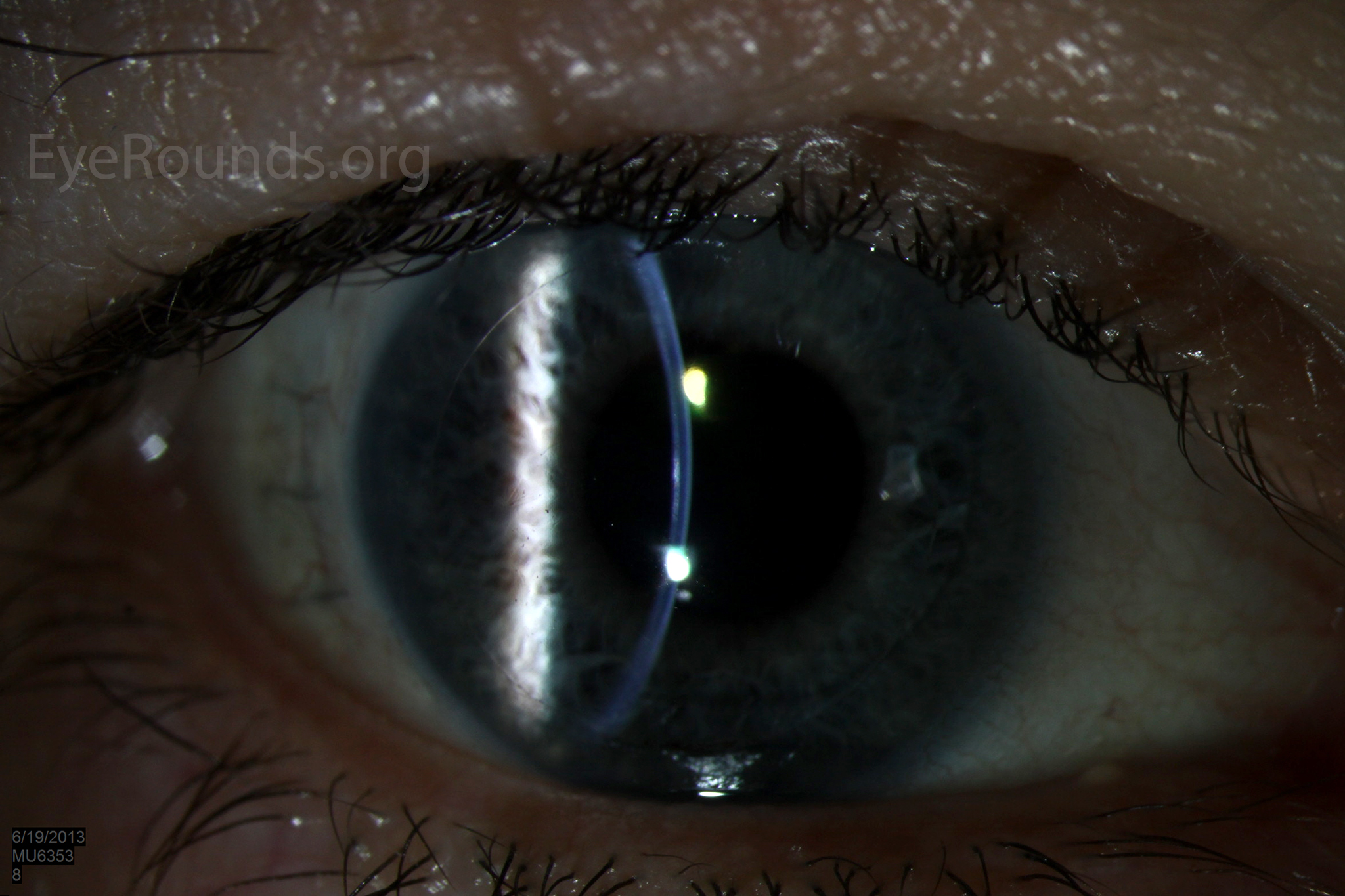
DSAEK is a partial thickness cornea transplant procedure that involves selective removal of the patient's Descemet membrane and endothelium, followed by transplantation of donor corneal endothelium in addition to donor corneal stroma (Figure 8). The transplanted tissue is approximately 100-200 microns thick. If the endothelium of the graft makes contact with any surgical instruments, it will be damaged and the graft may fail; therefore, the surgical procedure is designed to avoid contacting the donor endothelium. A tunneled corneoscleral incision is created, the recipient endothelium and Descemet membrane is removed, the graft is folded and inserted with non-coapting forceps (forceps that do not meet at the tips), and an air bubble is placed in the anterior chamber to support graft adherence. The procedure is used to treat corneal edema in the setting of endothelial dystrophies (such as Fuchs corneal dystrophy and posterior polymorphous corneal dystrophy), pseudophakic bullous keratopathy, iridocorneal endothelial (ICE) syndrome, endothelial failure in the setting of prior intraocular surgery or of a previous PK graft, and other causes of corneal endothelial dysfunction (1, 17-20).
 A |
 B |
 C |
 D |
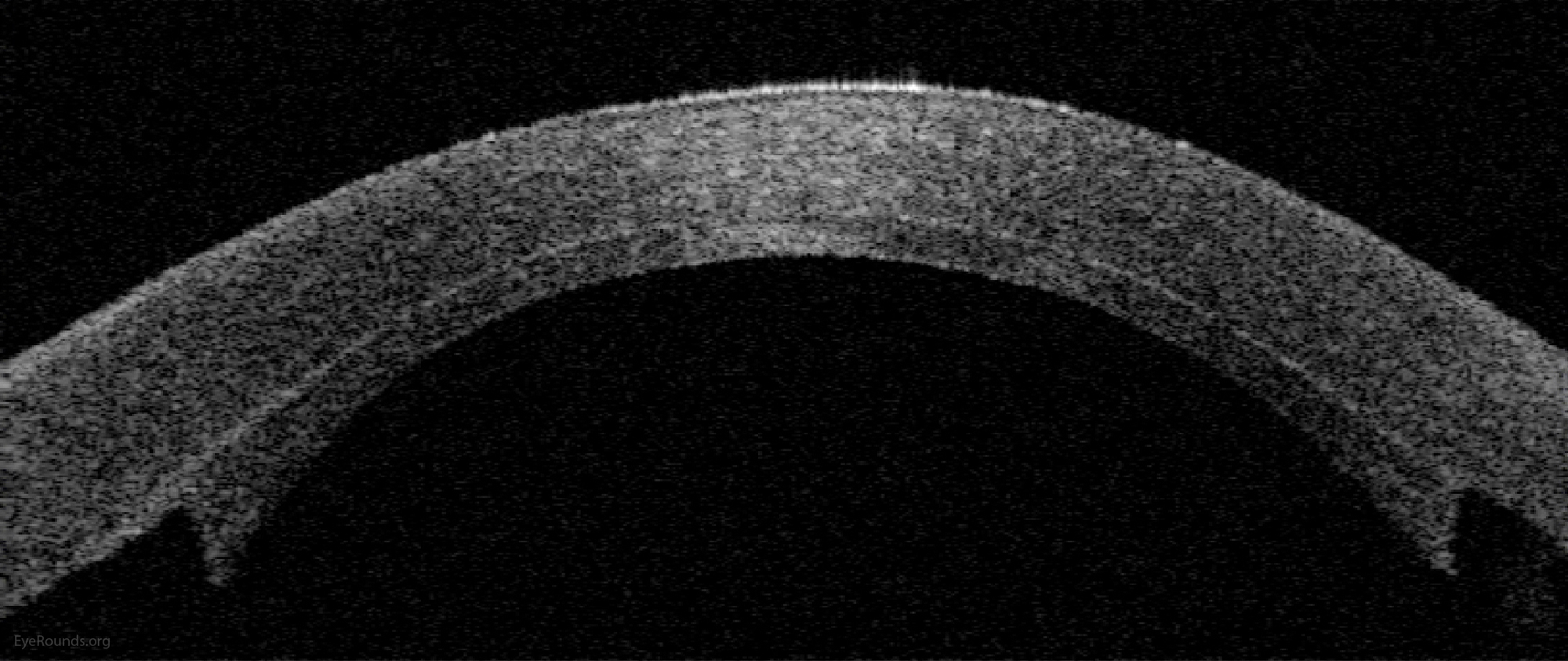
Figure 9: Anterior segment optical coherence tomography demonstrating an attached DSAEK graft one day after surgery.
DSAEK offers the advantage of relatively rapid healing time and visual rehabilitation. Compared to PK and DALK, there is less risk of graft rejection and suture-related complications. There is minimal topographic change to the corneal curvature. A somewhat predictable hyperopic shift results (typically 0.8-1.5 D), making intraocular lens selection easier when performing staged or simultaneous cataract surgery.
Postoperative visual acuity can be very good, but there is some limitation from the effects of the stroma-to-stroma graft-host interface. There is also a risk of postoperative graft dislocation.
Video 3: Descemet stripping automated endothelial keratoplasty (DSAEK) is an endothelial replacement procedure in which dysfunctional corneal endothelium is replaced with a graft consisting of donor endothelium and a thin layer of posterior stroma to facilitate handling of the tissue. This case was performed for severe corneal edema secondary to pseudophakic bullous keratopathy. Contributed by Jesse Vislisel, MD, and Mark A. Greiner, MD
Basic procedure steps (Video 3):
- Perform temporal peritomy and achieve hemostasis.
- Create a paracentesis and inject Healon into the anterior chamber.
- Make a 5 mm sclerocorneal tunnel; do not enter the anterior chamber.
- Use a bent 30-gauge needle and Sinskey hook to create an inferior peripheral iridotomy to prevent postoperative pupillary block.
- Place a marked circular ring of the planned donor size on the surface of the cornea to mark a template for resection of the patient's corneal tissue.
- Use a reverse Terry-Sinskey hook to score Descemet membrane just inside the ink marks previously made; strip it away from the stroma.
- Pass a keratome through the corneoscleral tunnel and into the anterior chamber.
- Remove the detached Descemet membrane using forceps.
- Roughen the peripheral stromal bed, outside the visual axis, using a Terry scraper to promote graft adhesion.
- Enlarge the wound to a full 5 mm width and then close it temporarily with a single interrupted 10-0 Vicryl suture.
- Remove the Healon from the anterior chamber using the I/A handpiece.
- Prepare the graft by trephinating the pre-cut donor tissue endothelial side up.
- Fold the donor tissue into a taco shape.
- Insert the donor tissue into the anterior chamber using non-coapting forceps.
- Unfold and float the donor graft using balanced salt solution (BSS), followed by air.
- Fill the anterior chamber with air to pressurize the eye.
- Use a Cindy sweeper to perform external compression on the surface of the cornea, first to position the graft if needed, and then to remove any central interface fluid.
- Close the temporal wound with 3 interrupted 10-0 Vicryl sutures.
- Leave the tissue undisturbed for 10-15 minutes to allow for adherence.
- Close the conjunctiva using cautery.
- Perform and air-fluid exchange to remove enough air from the anterior chamber to ensure there is no air behind the iris.
- Add air back into the anterior chamber to achieve a freely mobile bubble that covers the graft.
Additional Resources:
Video Links
- DSAEK with IOL Exchange (trans-scleral sutured method)
- Phakic DSAEK in a Child for Endothelial Dystrophy
- Combined Phacoemulsification and Descemet's Stripping Automated Endothelial Keratoplasty (DSAEK)
Articles