A 4-year-old boy was admitted for failure to thrive, worsening anorexia, and vomiting. Ophthalmology was consulted for evaluation of abnormal eye alignment. Medical history was significant for a 10q26 deletion, which involves the ARMS2 gene, in addition to hypotonia and developmental delay. Examination was significant for bilateral 6th nerve palsies with bilateral grade I disc edema.
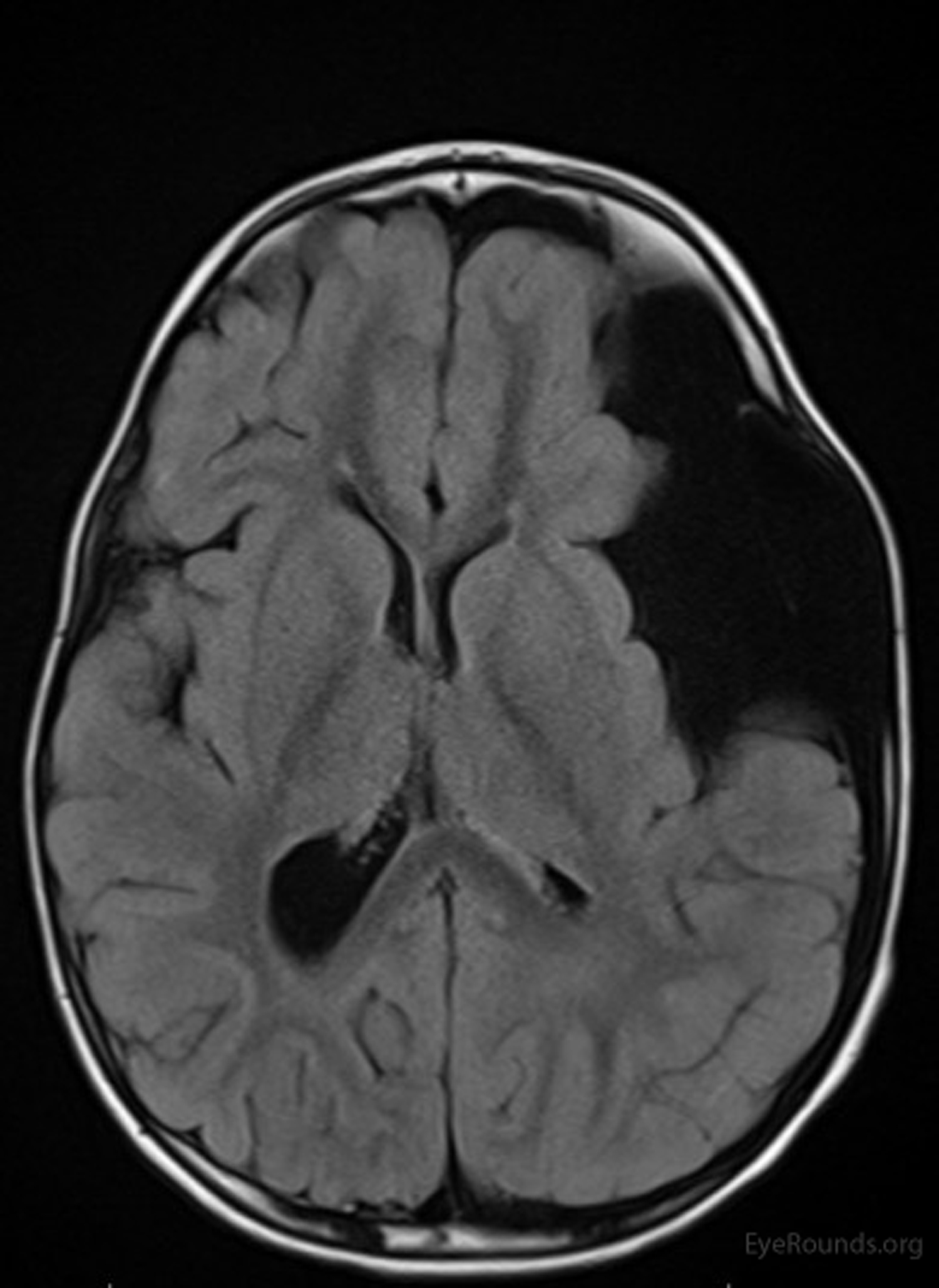
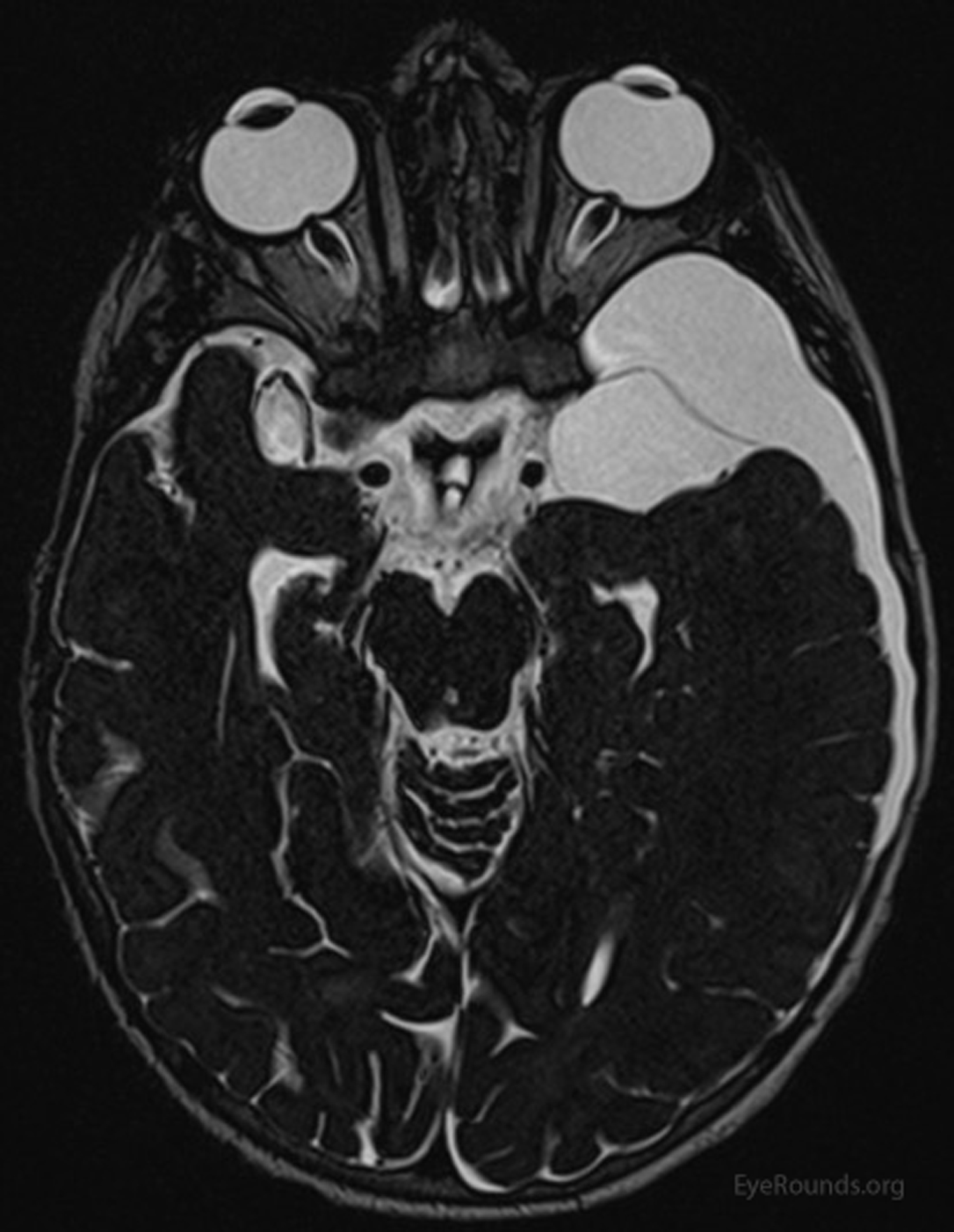
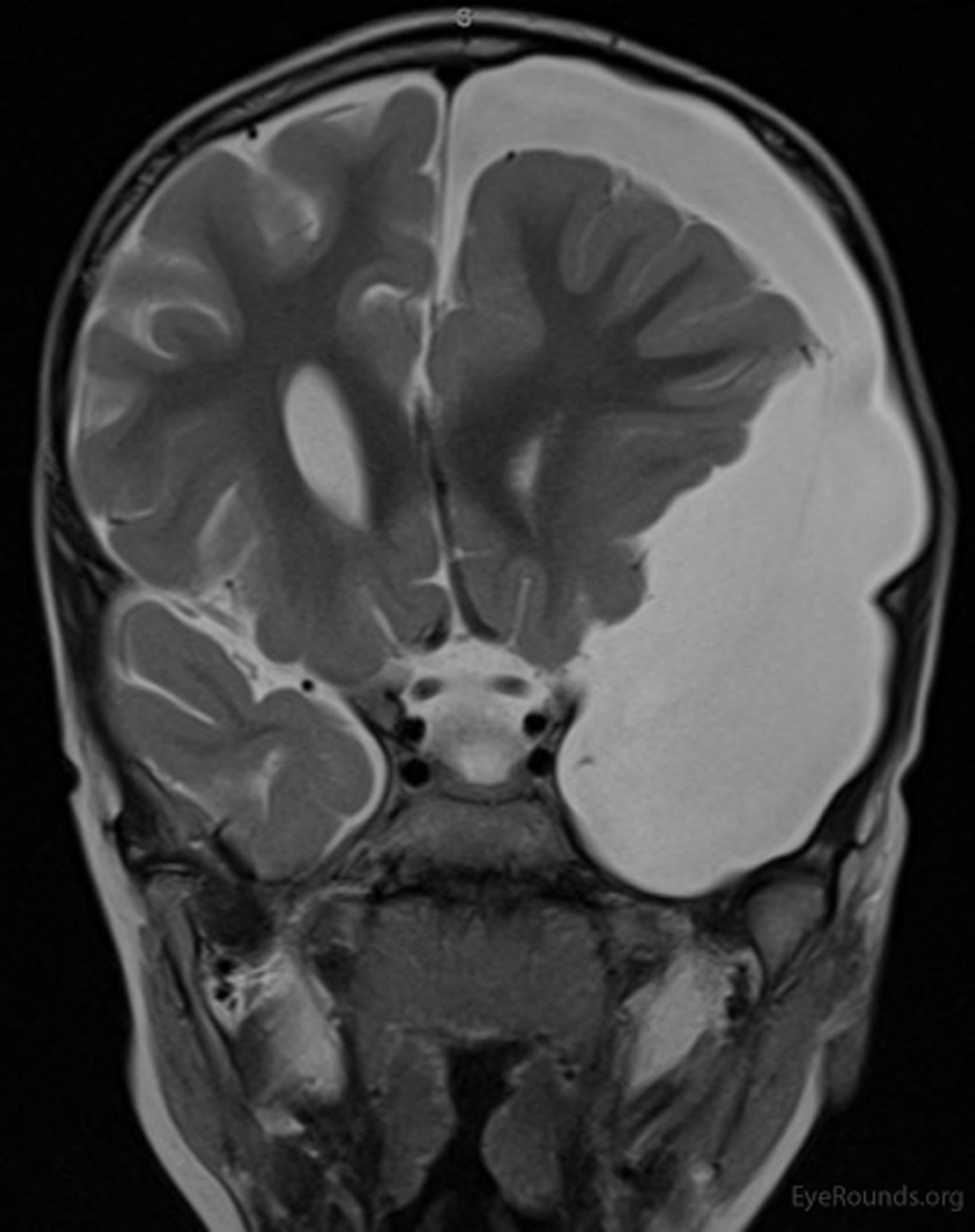
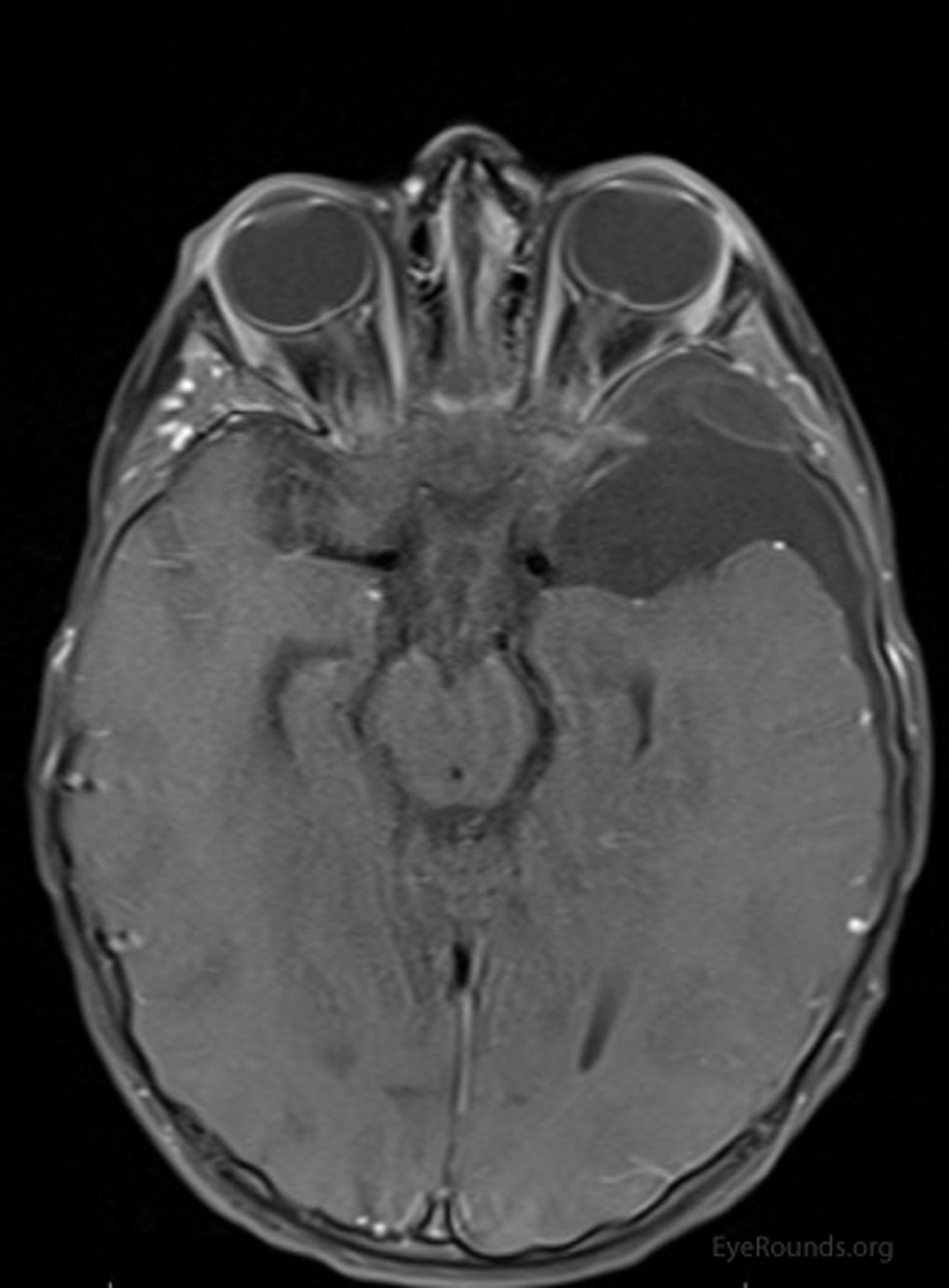
Magnetic resonance imaging (MRI) showed left-sided polymicrogyria and a large cystic lesion in the left temporal lobe (Figures 1-4) that appeared bright on T2-weighted imaging (Figure 1), was suppressed completely on FLAIR sequence (Figure 2), and had no post-contrast enhancement (Figure 3). These findings were consistent with an arachnoid cyst. Additionally, there was a 6 mm right midline shift with posterior globe flattening, protrusion of the optic nerve heads bilaterally, and mild prominence of the subarachnoid space of the bilateral optic nerves (Figure 4), consistent with increased intracranial pressure (ICP).
Arachnoid cysts, if large, can lead to displacement of neurovascular structures and increased ICP. Review of literature suggests that arachnoid cysts may be a rare cause of acquired sixth nerve palsy and strabismus in children [1]. Neurosurgical shunting followed by strabismus surgery relieved the abduction deficit and esotropia in several case reports [2]. This patient underwent a left cystoperitoneal shunt with improvement in his systemic symptoms. At his one month follow up appointment, he had normal ocular motility and alignment and his papilledema had resolved.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links