The University of Iowa
Department of Ophthalmology and Visual Sciences
February 27, 2005
ADMINISTERING LOCAL NERVE BLOCKS
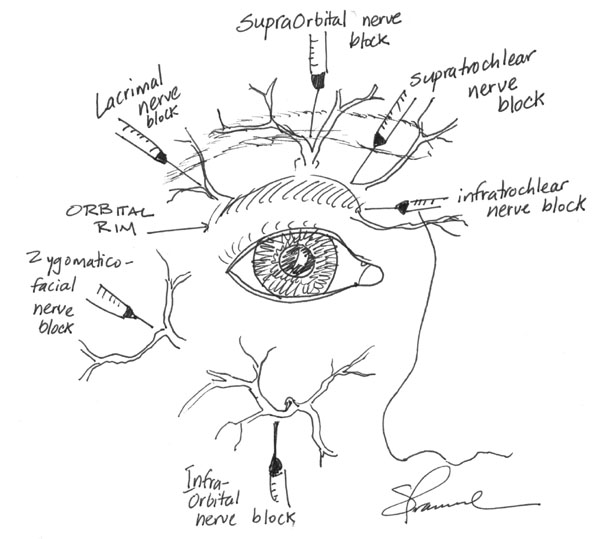
The most common local anesthetic mixture is 2% lidocaine with 1:100,000 epinephrine to provide some hemeostasis. Addition of 0.5% bupivacaine will provide longer anesthesia (~6-8 hours) for lengthy procedures. The following diagrams illustrate common local nerve blocks used in ophthalmology.
Diagram 1: Common Periorbital Nerve Blocks
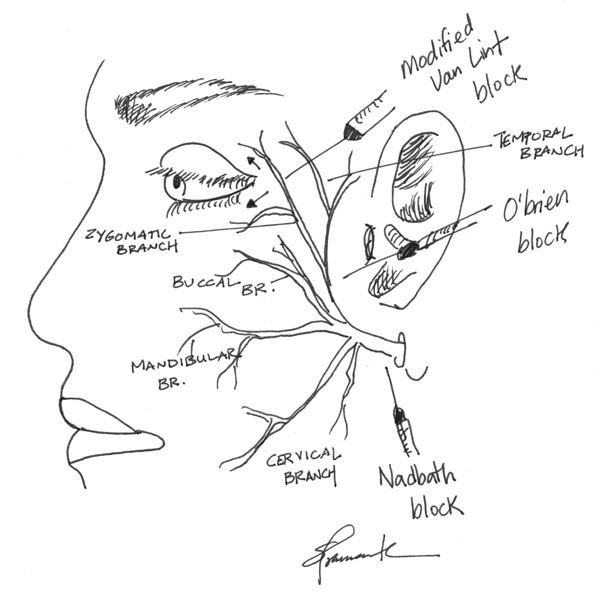
Diagram 2: Common Facial Nerve Blocks
ADMINISTERING THE RETROBULBAR BLOCK
Retrobulbar blocks are useful methods of achieving anesthesia for intraocular and orbital surgeries. Blocks are good alternatives to general anesthesia when general anesthesia is undesireable or contraindicated.
There are many techniques to adminster a retrobulbar block. The method described here is what I prefer. Depending on the type of anesthetic, a block may last over four hours with a mixture of lidocaine 1% and bupivicaine 0.375%. Addition of hyaluronidase to the anesthetic mix improves penetration of anethesia (Anesth Analg 2000 Oct;91(4):934-7.)
Clean the lower lid with an alcohol wipe.
Have the patient look straight ahead.
Use a 5 cc syringe and a 23 gauge, 1.5 inch flat grind needle.
Start 2/3 lateral along the inferior orbital rim (inferior to the temporal limbus) with the needle tip pointing perpendicular to the plane of the patient’s face. Place the index finger between the globe and the infraorbital rim, elevating the globe.
Stabilize with the little finger and hypothenar eminence firmly on the bones of the patient’s cheek.
Enter just inferior to the globe and perpendicular to the plane of the face.
Once you feel the first pop through the orbital septum, angle 45 degrees medially and 45 degrees superiorly towards the apex of the orbit until the second pop throught the muscle cone is felt.
Culver Boldt, MD (vitreoretinal surgeon) moves the needle gently side to side while advancing beneath the globe. If the needle begins to engage the globe, then the eye will start to move side to side. Hopefully, one can stop advancing before globe perforation occurs. This move is controversial, because some feel it leads to a higher rate of orbital hemorrhage.
John Sutphin, MD (corneal specialist) suggests watching for globe movement. The globe should rotate downward when you engage the septum. As you go through, it should rotate back up. Failure to do so could suggest the needle is in the sclera.
Pull back on the syringe to ensure the needle is not in a vessel, then inject 3-5 cc of anesthetic, palpating the globe to assess for posterior pressure.
After withdrawing the needle, apply firm pressure to the globe with a 4x4 gauze (enough to occlude the central retinal artery) to tamponade any possible retrobulbar hemorrhage. Provide firm pressure for 90-120 seconds. Some suggest alternating 10-15 seconds of firm pressure with release of the pressure to allow perfusion of the central retinal artery. Studies by Sohan Hayreh, MD, PhD (vascular) demonstrate that the retina is able to tolerate up to 90 minutes of non-perfusion before permanant damage.
Figure 2: Retrobulbar Block - Step 2 Pull back on the syringe to ensure the needle is not in a vessel, then inject 3-5 cc of anesthetic, palpating the globe to assess for posterior pressure.
Figure 3: Retrobulbar Block - Injection After withdrawing the needle, apply firm pressure to the globe with a 4x4 gauze (enough to occlude the central retinal artery) to tamponade any possible retrobulbar hemorrhage. Provide firm pressure for 90-120 seconds. Some suggest alternating 10-15 seconds of firm pressure with release of the pressure to allow perfusion of the central retinal artery. Studies by Sohan Hayreh, MD, PhD (vascular) demonstrate that the retina is able to tolerate up to 90 minutes of non-perfusion before permanant damage.
ADMINISTERING THE SUB-TENONS PERIBULBAR BLOCK
A peribulbar block is an alternative to the retrobulbar block and offers an effective way to provide anesthesia before ocular surgery (Br J Ophthalmol. 1997 Aug;81(8):673-6).
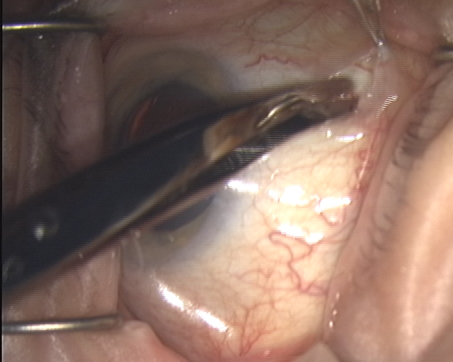
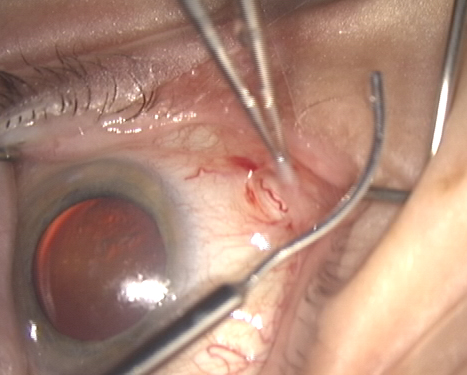
A small button hole is made in the conjunctivae and tenons using Westcott scissors and 0.12 forceps (Figure 4).
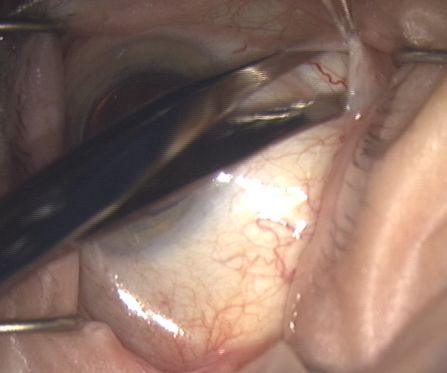
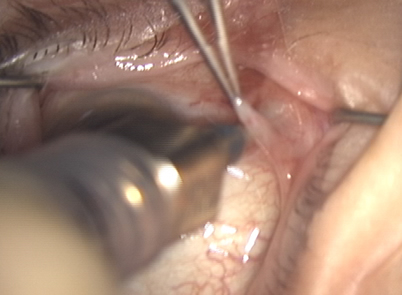
The quadrant is freed using blunt dissection with Westcott scissors (Figure 5).
1% lidocaine/0.375% bupivacaine is drawn up in a syringe attached to a blunt lacrimal cannula (Figure 6) and then inserted posteriorly under the sub-tenons space (Figure 7).
Figure 4: Button hole formed ~10 mm from the corneal limbus. A peribulbar block is an alternative to the retrobulbar block and offers an effective way to provide anesthesia before ocular surgery (Br J Ophthalmol. 1997 Aug;81(8):673-6).
A small button hole is made in the conjunctivae and tenons using Westcott scissors and 0.12 forceps (Figure 4).
Figure 5: Freeing the Quadrant The quadrant is freed using blunt dissection with Westcott scissors (Figure 5).
Figure 6: Lacrimal cannula 1% lidocaine/0.375% bupivacaine is drawn up in a syringe attached to a blunt lacrimal cannula (Figure 6)
Figure 7: Insertion of cannula(a) and injection of anesthetic(b). inserted posteriorly under the sub-tenons space (Figure 7).
Figure 7: Insertion of cannula(a) and injection of anesthetic(b). inserted posteriorly under the sub-tenons space (Figure 7).
Suggested citation format
Pramanik S, Doan A. Retrobulbar Block, Peribulbar Block, and Common Nerve Blocks Used by Ophthalmologists. February 27, 2005; Available from https://eyerounds.org/tutorials/retrobulbar-nerve-blocks.htm
University of Iowa
Roy J. and Lucille A. Carver College of Medicine
Department of Ophthalmology and Visual Sciences
200 Hawkins Drive
Iowa City, IA 52242
University of Iowa
Roy J. and Lucille A. Carver College of Medicine
Department of Ophthalmology and Visual Sciences
200 Hawkins Drive
Iowa City, IA 52242