The University of Iowa
Department of Ophthalmology and Visual Sciences
Initial posting date: May 24, 2018
Objectives
Identify orbital and eyelid anatomy associated with orbital compartment syndrome and lateral canthotomy/cantholysis.
Describe the signs of orbital compartment syndrome and evaluation for lateral canthotomy/cantholysis.
Describe the steps of lateral canthotomy/cantholysis
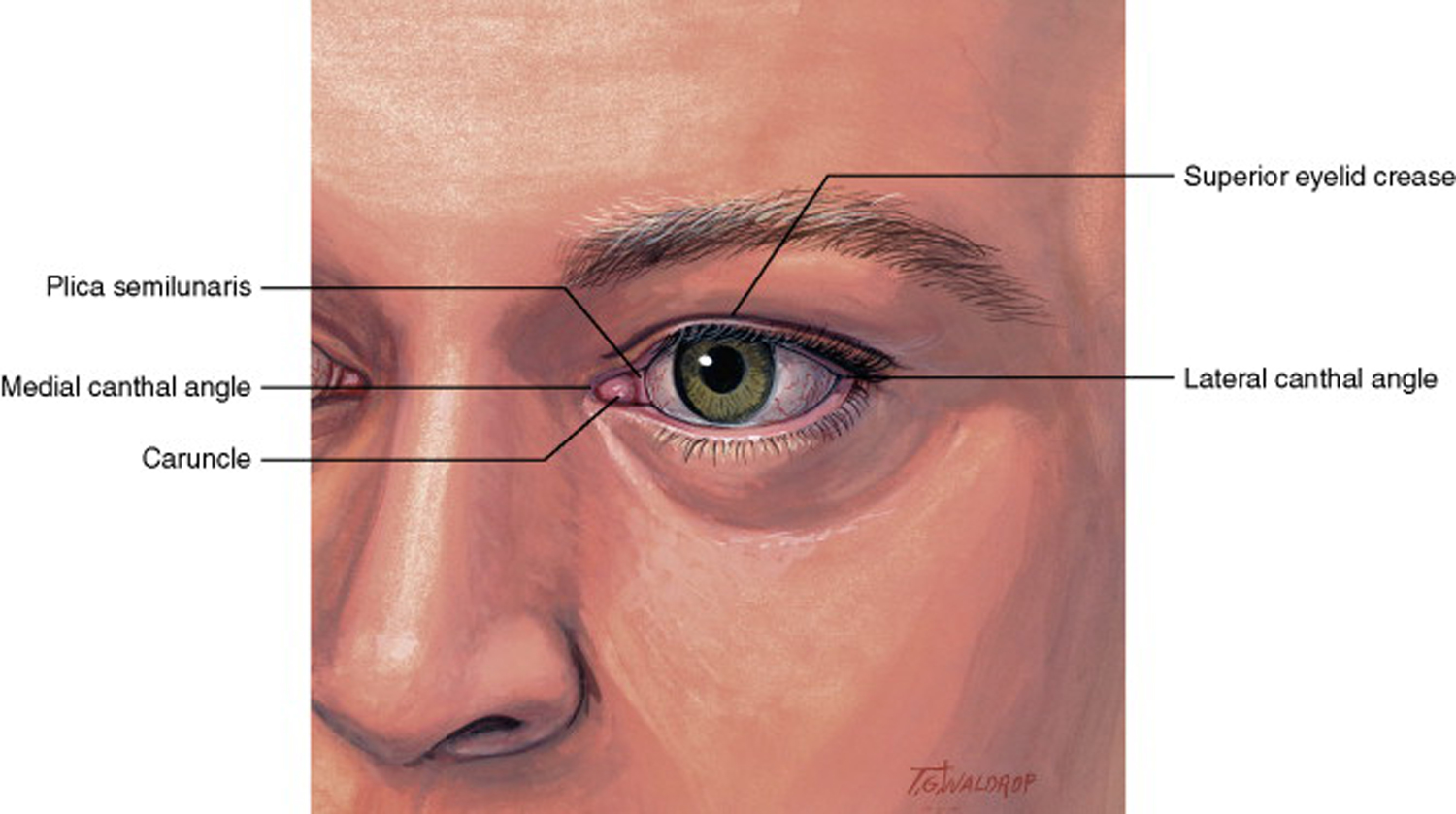
Figure 1: External eyelid anatomy with the lateral canthal angle at the point where the upper and lower eyelids meet. (Reprinted with permission from Elsevier.) [1]
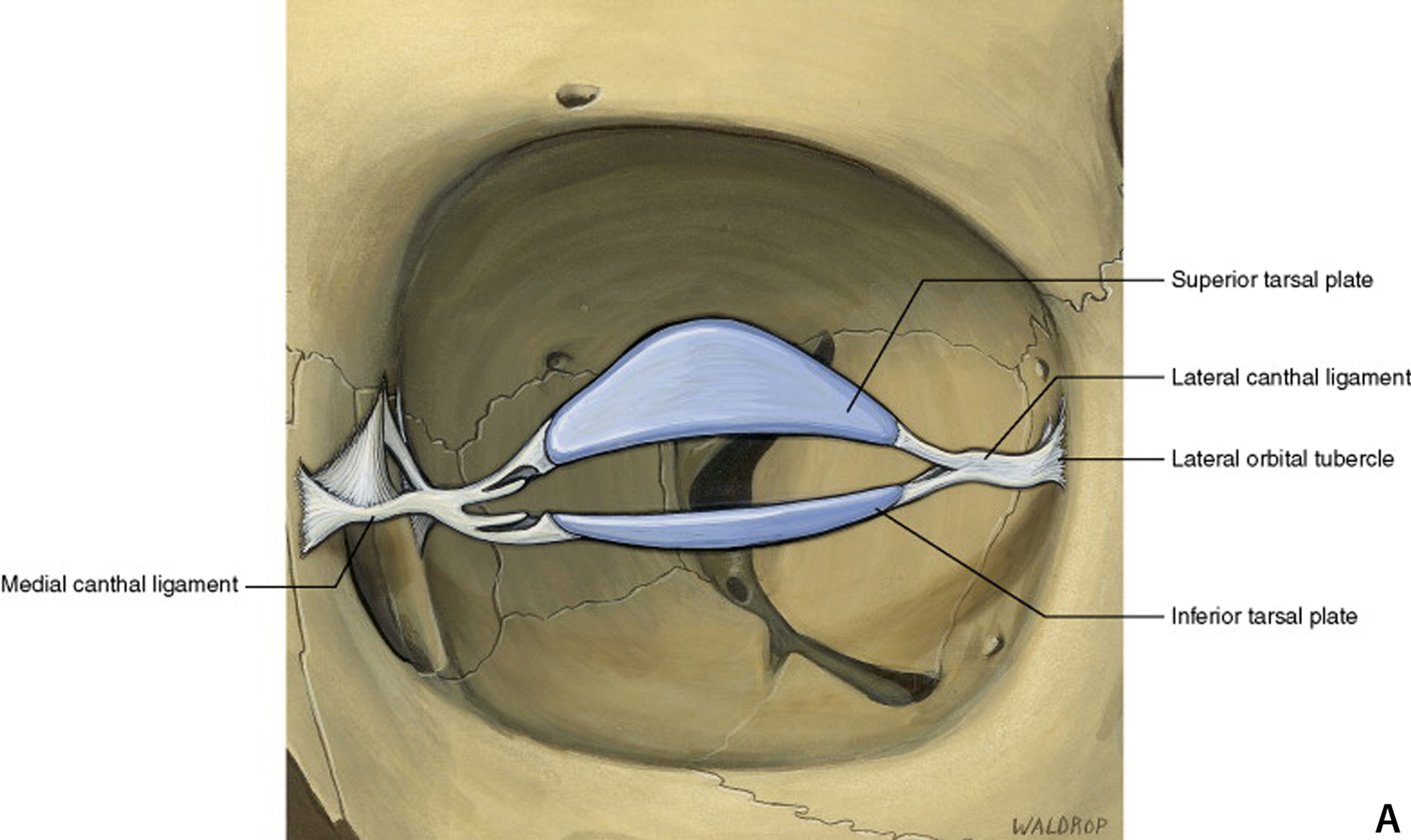
Figure 2a: Lateral canthal tendon attaches the tarsal plates of the eyelid to the periosteum at the lateral orbital tubercle. (Reprinted with permission from Elsevier.) [1]
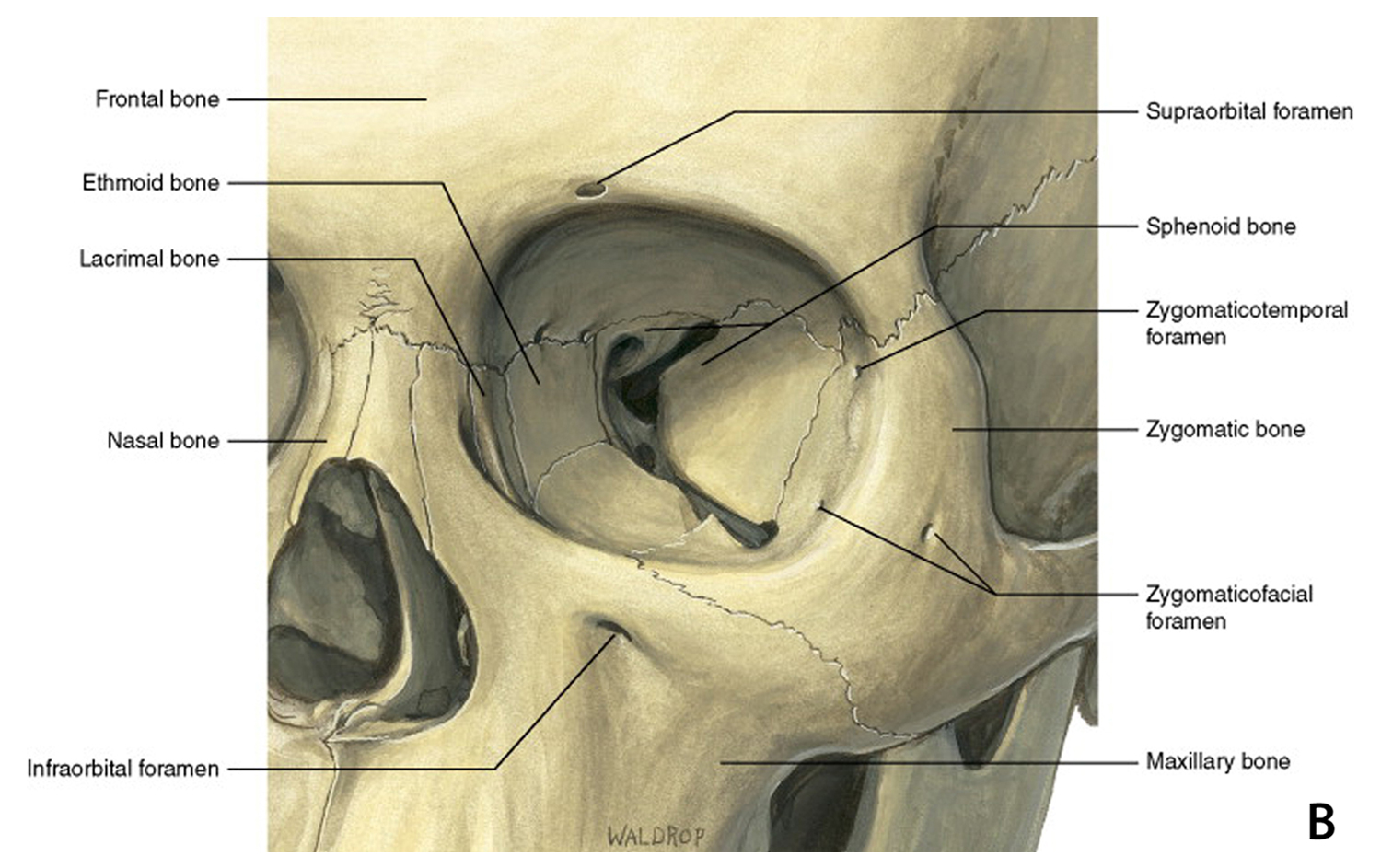
Figure 2b:The orbital compartment is a closed compartment and the walls are comprised of 7 bones, including the ethmoid, lacrimal, sphenoid, frontal, maxillary, zygomatic, and palatine bones. (Reprinted with permission from Elsevier.) [1]
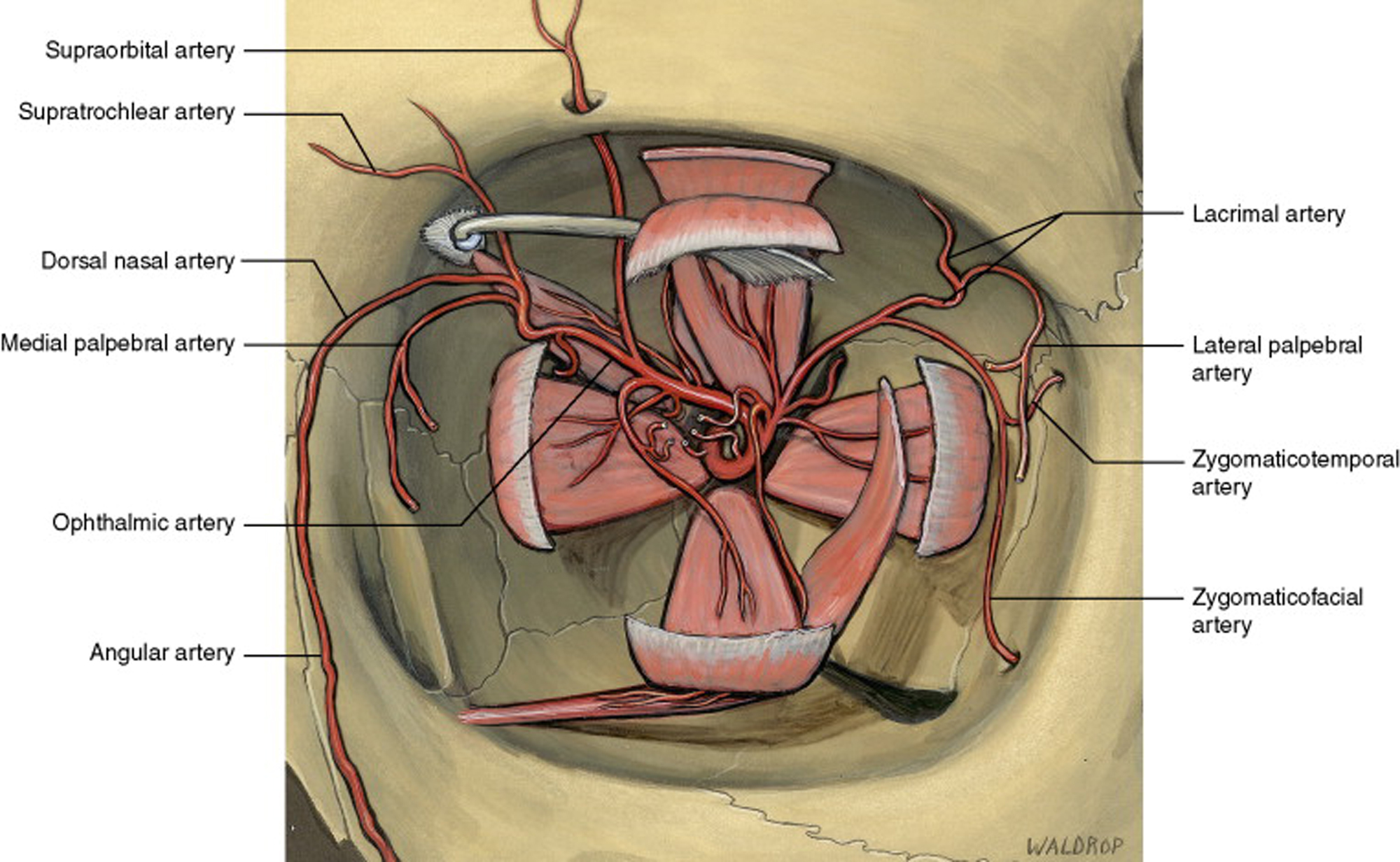
Figure 3: Orbital arteries with extraocular muscles. The primary blood supply to the orbit comes from the ophthalmic artery. The ophthalmic artery is a branch of the internal carotid artery and has many branches to supply the ocular tissue, optic nerve, and the orbit. (Reprinted with permission from Elsevier.) [1]
Evaluation for Canthotomy/Cantholysis
Orbital compartment syndrome refers to a situation in which an expansile process within the closed compartment of the orbit leads to increased orbital pressure, which can further lead to ischemia and vision loss. The diagnosis of orbital compartment syndrome is made based on clinical findings and should be suspected in patients presenting with the following constellation of symptoms: acute proptosis, elevated intraocular pressure (35-40 mmHg), rapid vision loss, ophthalmoplegia, and fixed dilated pupils or a relative afferent pupillary defect (RAPD).
Orbital compartment syndrome requires immediate treatment to prevent permanent vision loss. Time to intervention should be within 90-120 min from injury to prevent vision loss (based on primate studies) [2].
Etiology
Any expansile process within the orbit can lead to orbital compartment syndrome. These include:
Retrobulbar hemorrhage
Trauma
Vascular malformations/tumors
Cellulitis/infection
Extravasation of dyes/contrast/fluid (burn)
Orbital malignancy
Orbital surgery
Increased risk with anticoagulant use and/or bleeding disorders
Pathophysiology
Increased orbital pressure causes anterior displacement of the globe →
Anterior displacement of the globe is limited by the eyelid complex which is anchored to the orbital rim by the lateral and medial canthal tendons→
The orbit follows pressure-volume dynamics similar to other compartment syndromes: Increased tissue pressure in an enclosed space leads to decreased perfusion. When the intraorbital pressure exceeds arterial pressure supplying the optic nerve and retina, ischemia results.
The central retinal artery may have some protection from direct compression because of its anatomic position within the optic nerve and because of its higher systolic pressure, but it is still at risk for compression in orbital compartment syndrome
Lower pressure capillaries and the posterior ciliary arteries, which enter the eye around the optic nerve, are afforded no such protection and ischemia of these vessels leads to vision loss due to ischemic optic neuropathy
Stretching of the optic nerve and vessels can also result in vision loss.
Signs of orbital compartment syndrome
Elevated intraocular pressure (>35mmHg)
Decreased vision
Relative afferent pupillary defect or a fixed, dilated pupil
Restricted extraocular motility (ophthalmoplegia)
Acute proptosis with taut lids
Computed Tomography (CT) Scan: globe tenting, proptosis, presence of retro-orbital hemorrhage/edema/or mass lesions
Assessing for signs of orbital compartment syndrome
Goal: To disinsert lateral canthal ligaments from the orbital rim in order to allow anterior displacement of the globe, leading to a reduction in intraorbital pressure and a return of optic nerve and retinal circulation
Steps:
Assess the status of the affected eye. Generally, lateral cantholomy/cantholysis are contraindicated when the eye is lacerated or ruptured. If the eye is intact, proceed with lateral canthotomy/cantholysis.
Apply local anesthetic (Commonly lidocaine 2% with epinephrine 1:100,000)
Clean, Sterilize (i.e.Povidine-iodine), and drape the eye and lateral canthal area
Use non-dominant hand to hold traction on the lateral eyelids
Use scissors (Utility, Stevens or Westcott) to create canthotomy at the lateral orbital rim
Use forceps to apply downward traction on lower lid
Use scissors to perform inferior cantholysis - palpate and "strum" the inferior crus of the lateral canthal tendon and cut
Recheck pressure
If inferior cantholysis is insufficient, consider release of the superior crus in a similar manner as the inferior crus was released. Care should be taken to avoid the lacrimal gland and its ductules.
Tse DT. A Simple Maneuver to Reposit a Subluxed Globe. Arch Ophthalmol. 2000;118(3):410–411.
Suggested citation format
Stiff HA, Chung AT, Benage M, Janson BJ, Fox AR, Oetting TA, Shriver EM. Orbital Compartment Syndrome Curriculum. EyeRounds.org. Posted September 4, 2018; Available from: https://eyerounds.org/tutorials/ocs/index.htm
University of Iowa
Roy J. and Lucille A. Carver College of Medicine
Department of Ophthalmology and Visual Sciences
200 Hawkins Drive
Iowa City, IA 52242
University of Iowa
Roy J. and Lucille A. Carver College of Medicine
Department of Ophthalmology and Visual Sciences
200 Hawkins Drive
Iowa City, IA 52242