INITIAL PRESENTATION
Chief Complaint: Difficulty with low-light vision and glare.
History of Present Illness:
A 73-year-old male with an ocular history of bilateral laser in-situ keratomileusis (LASIK) and several subsequent enhancement procedures presented for a cataract evaluation. He reported significant issues with driving, especially at night or towards bright lights, as well as mild ocular surface dryness in both eyes (OU).
Past Ocular History:
Past Medical History:
Medications:
Allergies:
Family History:
Social History:
Review of Systems:
OCULAR EXAMINATION
| OD | OS | |
|---|---|---|
| Lids/Lashes | small, elevated red vascularized lesion on the upper lid near margin, fleshy papule near lateral canthal region; inferior scleral show | normal |
| Conjunctiva/Sclera | temporal and nasal pinguecula | temporal and nasal pinguecula |
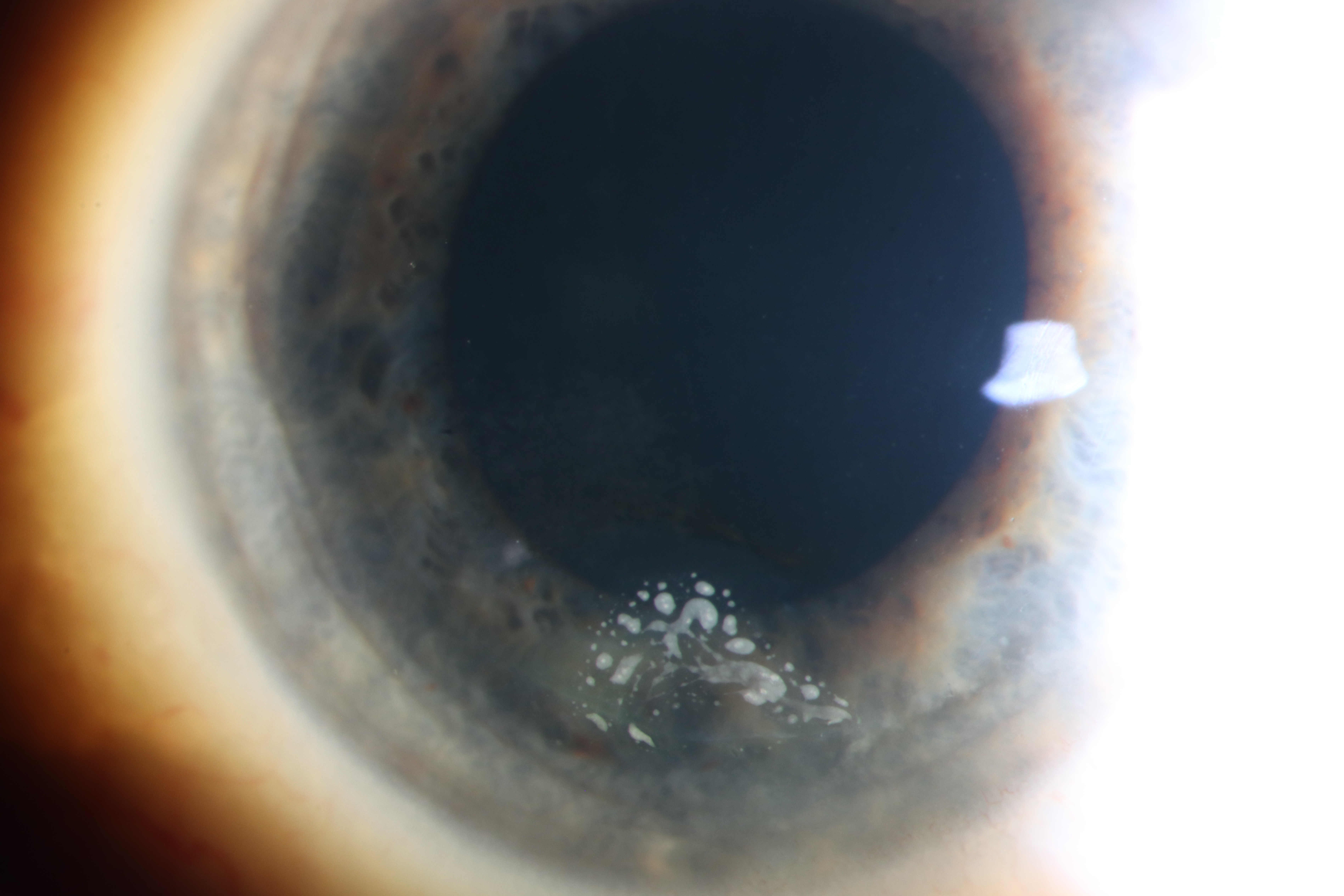
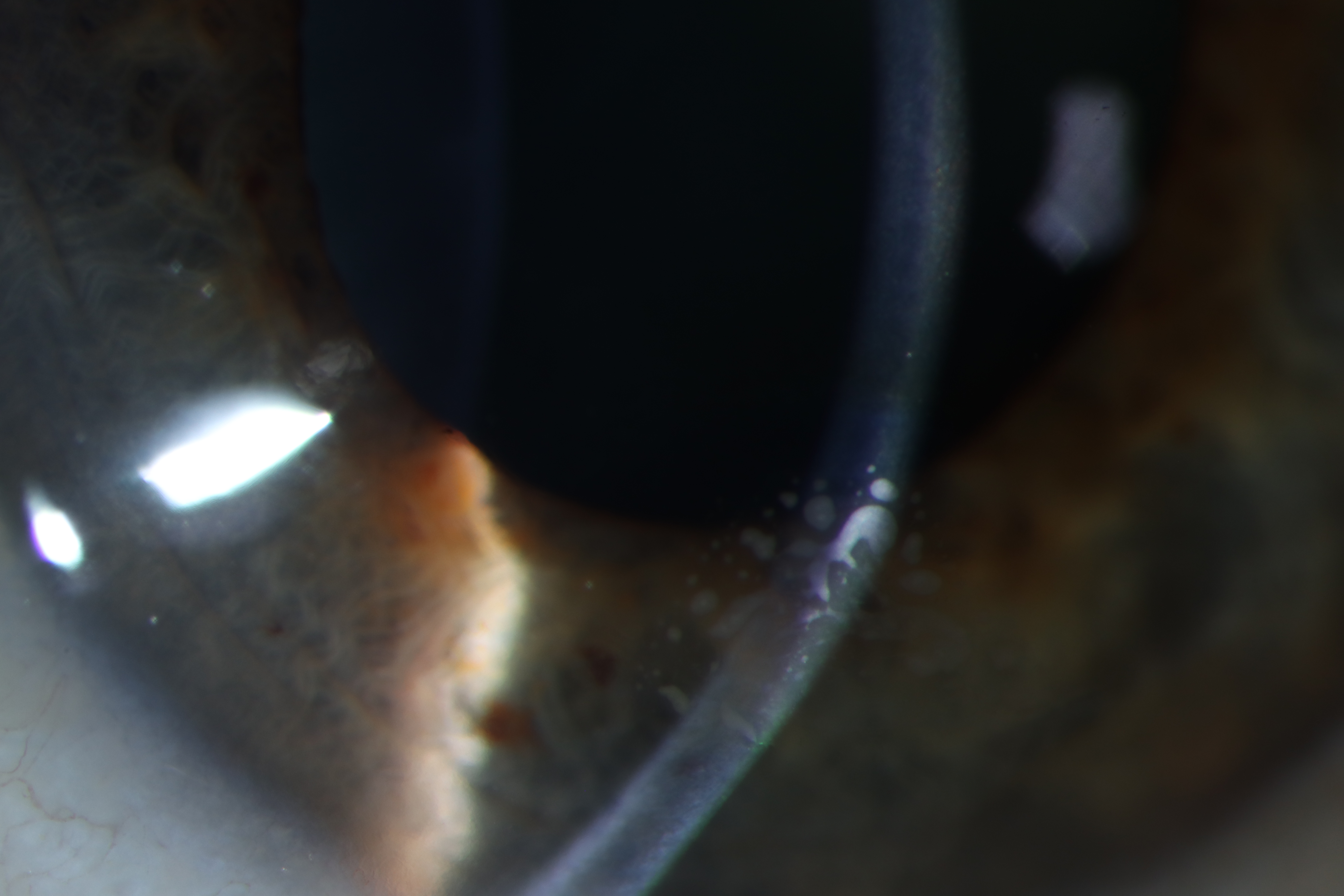
| Cornea | small triangular cluster of subepithelial dense opacities inferiorly, LASIK flap well-centered and without evidence of infiltrate, rapid tear breakup time (about 4 seconds) | small circular epithelial opacities superiorly, LASIK flap well-centered and without evidence of infiltrate, rapid tear breakup time (about 4 seconds) |
| Anterior Chamber | deep and quiet | deep and quiet |
| Iris | normal architecture, no transillumination defects | normal architecture, no transillumination defects |
| Lens | 1+ nuclear sclerosis | 1+ nuclear sclerosis |
CLINICAL COURSE
In summary, the patient was noted to have a hyphema, disc hemorrhage, traumatic mydriasis, reactive ptosis, and peripapillary commotio retinae in the left eye secondary to blunt force trauma. He had no evidence of an open globe injury and sickle screening was negative. Thus, the patient was discharged on cyclopentolate 1% drops twice daily, and prednisolone acetate 1% four times daily, and returned to the eye clinic the following day for follow up and intraocular pressure check.
DIAGNOSIS: Epithelial ingrowth of the right eye.
DISCUSSION
Pathophysiology
In the context of corneal refractive surgery, epithelial ingrowth (EI) is a rare complication characterized by the opportunistic infiltration of proliferating corneal epithelial cells into the stroma. There are two primary mechanisms in which epithelial cells infiltrate the stroma. During flap creation, isolated pockets of epithelial cells can be implanted under the flap but far from the flap edge. These nests are typically unable to proliferate due to separation from their normal ocular surface environment, resulting in minimal symptoms.(1) The other, more consequential mechanism of EI involves the introduction of a communicating pathway between the epithelial layers outside the flap and stromal bed under the flap. This is typically established because of poor flap adhesion, flap dislocation, or the presence of foreign bodies in the LASIK flap interface.(1, 2) Surgeons today use surface ablation procedures more frequently than flap lifts for LASIK enhancements due to the risk of EI.
Signs/Symptoms
Presentation of post-LASIK EI is remarkably variable in terms of severity, location, and progression. Symptomatically, visual acuity can be affected if EI colony fibrosis impinges on the visual axis or if flap deformation induces significant irregular astigmatism. Pain and irritation can arise from corneal insults such as corneal erosions, epithelial defects, or keratolysis[MKS1].(3)
Wang and Maloney describe four key clinical features for post-LASIK EI that can be found on slit lamp exam, including the presence of epithelial pearls in the flap interface, fluorescein pooling around an elevated flap, a fibrotic demarcation line, and melting of the flap edge.(1, 3) Other signs, such as a rolled flap edge and peripheral stromal haze, may also be present. The severity of EI is described by the Probst/Machat classification system, which grades based on clinical signs and progressive ingrowth towards the visual axis.(1)
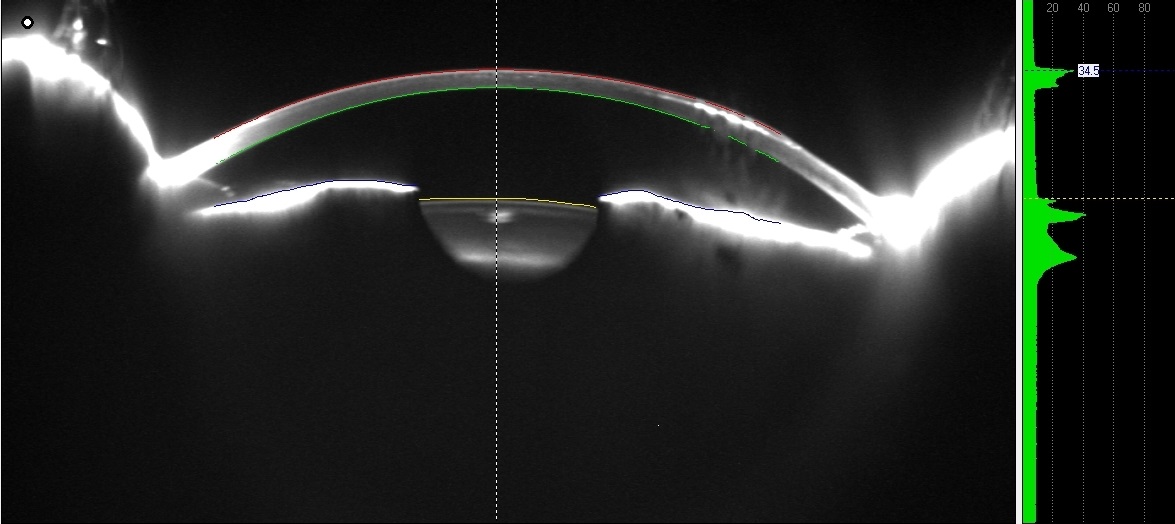
Imaging
Anterior segment optical coherence tomography (AS-OCT) and corneal densitometry can be used to detect subtler corneal changes that are not immediately evident at the slit lamp. Corneal topography can also be used to assess refractive changes induced by EI.(1)
Treatment/Management/Guidelines
The first step in management is determining the stability of the EI nest. If it is unchanging, not affecting visual acuity, and structurally intact, careful observation is reasonable. Simple mechanical debridement of the epithelial ingrowth followed by flap repositioning is the recommended intervention for epithelial ingrowth. Secure flap adhesion may further be facilitated by adjuvant surgical procedures, such as flap suturing, flap gluing, or the use of a hydrogel sealant on the flap’s edge.(1) Post-operative placement of bandage contact lens is generally recommended to protect the flap in its new position, but some small studies (n=30 eyes) have suggested that placement in a bandage lens may increase chance of re-epithelialization.(1, 4)
The recurrence rate of EI after treatment is estimated to be as high as 36%, which may necessitate repeat debridement and flap lift. In such refractory cases, antimetabolite therapies such as amniotic membrane graft placement or Mitomycin C therapy can be implemented to limit the rate of errant epithelial proliferation. In eyes unable to tolerate further surgeries, Nd:YAG laser ablation has been suggested as a novel non-invasive alternative, although current data is limited. Overall, over 40% of patients with recurrent EI require repeat procedures for complete elimination.(1)
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Mascardo C, Tomlinson LA, Matharu KS. Epithelial Ingrowth after LASIK . EyeRounds.org. May 28, 2026. Available from https://EyeRounds.org/cases/379-epithelial-ingrowth-after-LASIK.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links