INITIAL PRESENTATION
Chief Complaint: Bilateral ocular pain and photophobia
History of Present Illness:
Patient is a 46-year-old male with a past medical history significant for atopy (asthma, eczema, allergic rhinitis) and past ophthalmic history significant for multiple herpes simplex keratitis episodes who was referred to the University of Iowa for bilateral herpes keratitis. He was diagnosed three weeks prior by his local ophthalmologist and was refractory to treatment with topical Moxifloxacin 0.5% 1 drop four times daily in both eyes, Trifluridine 1 drop every two hours while awake in both eyes, Ganciclovir 1 drop 5 times daily in both eyes, and Valacyclovir 1000mg TID by mouth. Symptoms continued to worsen, so he was referred to the University of Iowa, with progressive bilateral stabbing eye pain and photophobia rendering him debilitated and house-bound. On presentation his right eye was more symptomatic than left.
Past Ocular History:
Past Medical History:
Medications:
Allergies:
Family History:
Social History:
Review of Systems:
OCULAR EXAMINATION
| OD | OS | |
|---|---|---|
| Lids/Lashes | Reactive upper eyelid ptosis, erythema of lid margin, mild meibomian gland dysfunction, blepharitis | Reactive upper eyelid ptosis, erythema of lid margin, mild meibomian gland dysfunction, blepharitis |
| Conjunctiva/Sclera | Diffuse trace injection | Diffuse trace injection |
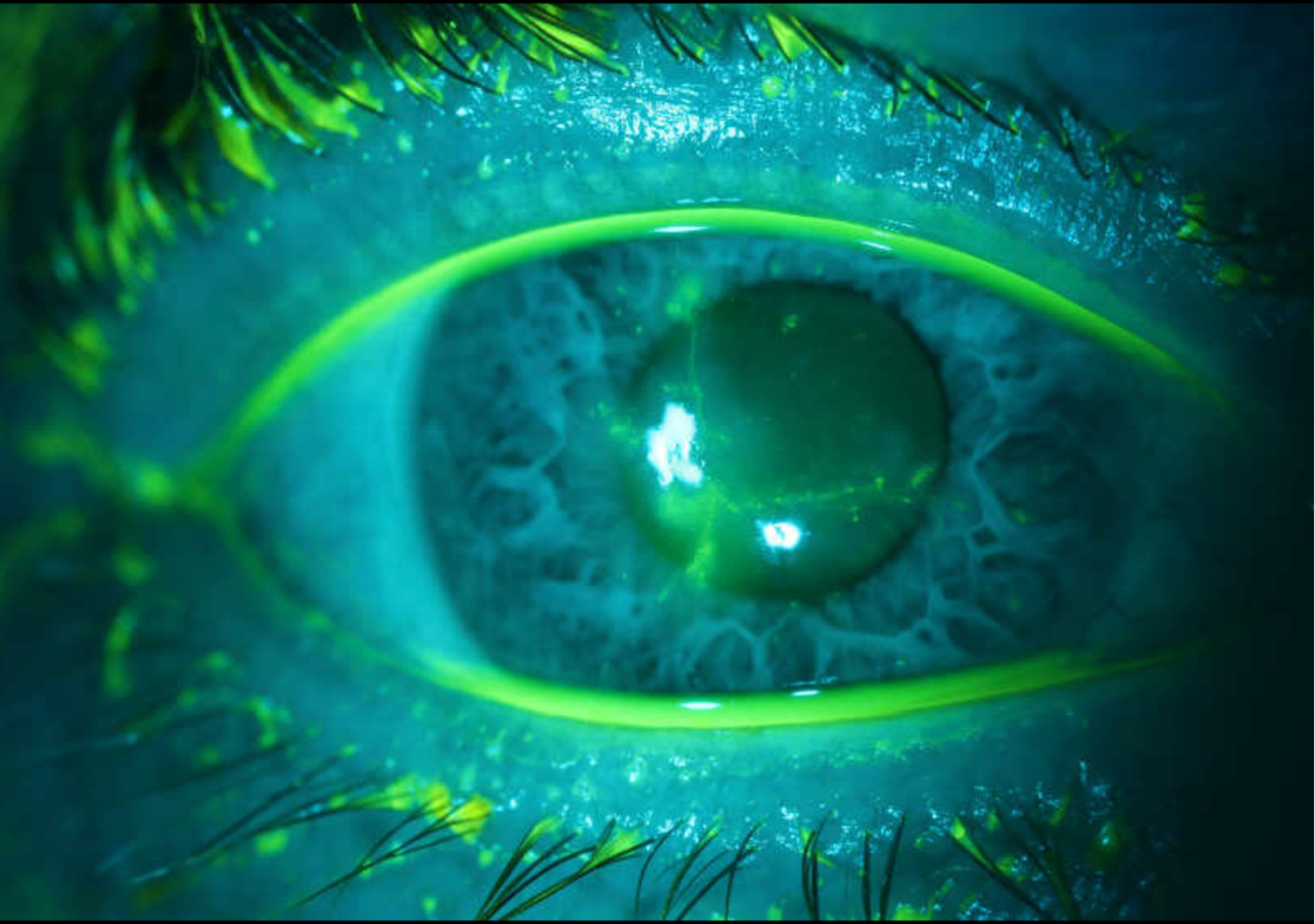
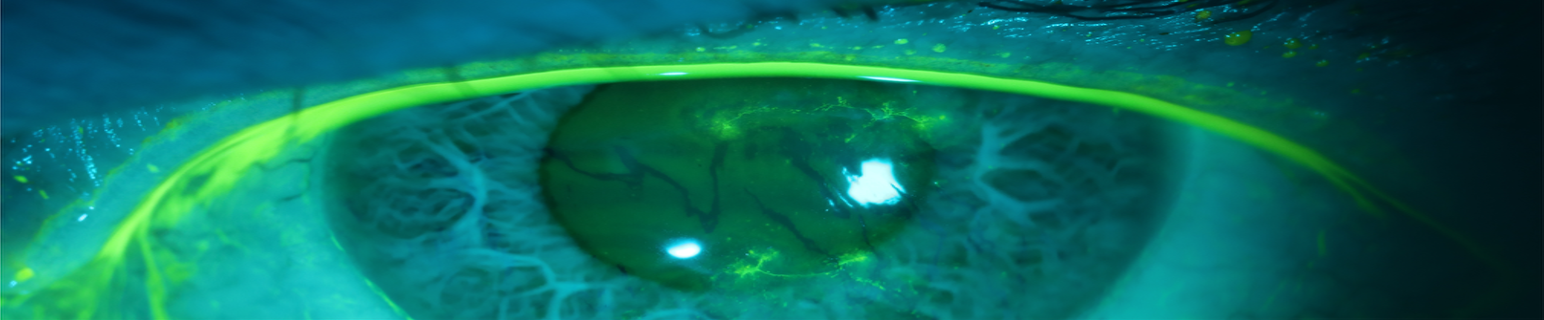
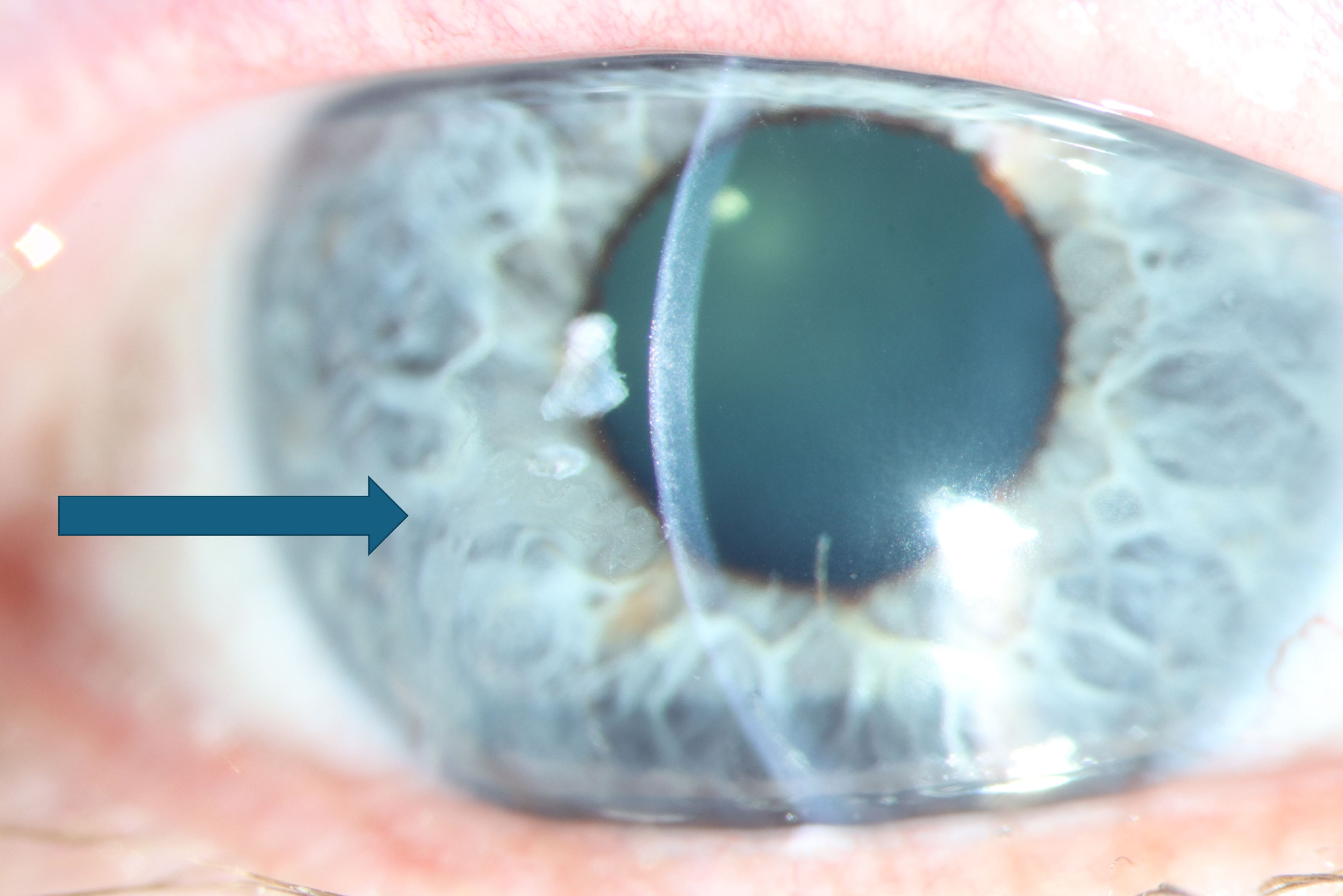
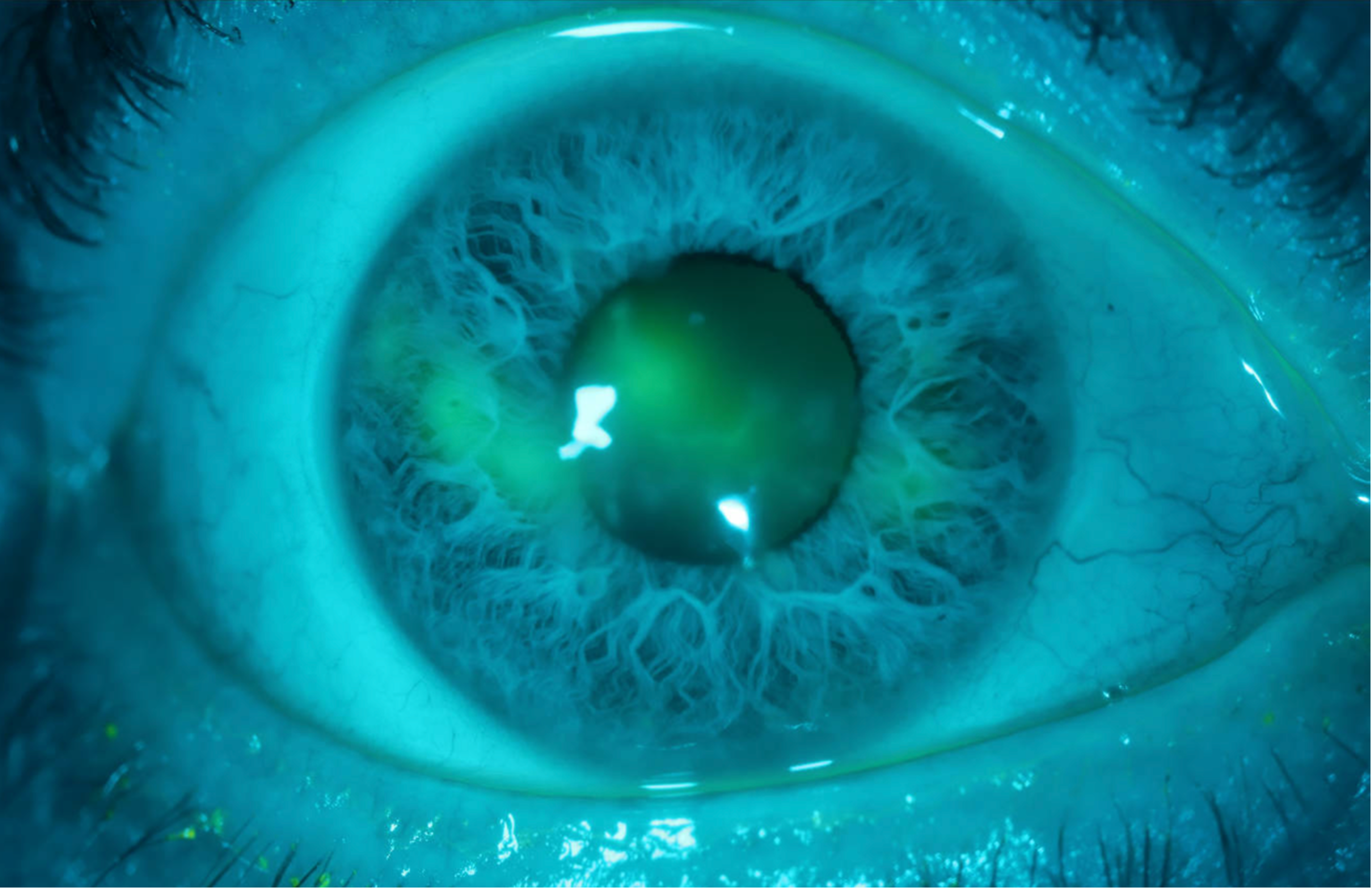
| Cornea | Large central confluent geographic ulcer. Some surrounding anterior stromal whitening (scarring vs edema). | Multiple short, linear epithelial defects without clear terminal bulbs |
| Anterior Chamber | Deep and quiet, no cell or flare | Deep and quiet, no cell or flare |
| Iris | Normal architecture, no iris defects | Normal architecture, no iris defects |
| Lens | Clear | Clear |
| Anterior and posterior Vitreous | Normal, no cell or snowbanking | Normal |
| Disc | Both eyes normal |
|---|---|
| Cup-to-disc ratio | Both eyes 0.0 |
| Macula | Both eyes normal |
| Vessels | Both eyes normal |
| Periphery | Both eyes normal, no retinal whitening |
DIFFERENTIAL DIAGNOSIS:
CLINICAL COURSE
His PCP obtained blood work prior to presentation, which showed positive VZV IgG and negative HSV-1 and HSV-2 IgG. Beyond his allergic rhinitis, there were no other signs of immunocompromised status. Corneal scraping of the right eye yielded a sample for PCR which was negative for HSV, VZV, and acanthamoeba. Tear sample PCR performed the same day was also negative for HSV.
A week later, symptoms slightly improved, however, dendritiform lesions persisted. ID was consulted and a CMV culture obtained from both eyes was negative. The leading diagnosis at this time was bilateral HSK due to tachyphylaxis or resistance to acyclovir from previous HSK episodes. The patient was admitted for IV acyclovir and was found to have an IgG deficiency. IVIG was thus added to the IV acyclovir treatment. Vision and all symptoms improved post treatment however photophobia persisted. The patient had a peripherally inserted central catheter (PICC) line placed and was discharged home on Acyclovir 750mg TID IV. Two weeks later, outpatient ID discontinued IV acyclovir and began Acyclovir 1500mg TID PO. Allergy next evaluated the patient and found transient hypogammaglobulinemia as well as decreased Natural Killer (NK) cell activity in response to IL-2. In addition, an inborn error of immunity and cytopenias panel was ordered which identified one likely pathogenic variant in 1 of 2 copies of the gene TNFRSF13B. This gene is associated with autosomal recessive common variable immunodeficiency (CVID). Possessing only 1 mutated copy is considered insufficient to cause disease; however, there are reports in the medical literature of patients with only 1 mutated copy ultimately developing CVID later in life. The Pneumovax vaccine was given with scheduled follow up to monitor immune response.
One week later, ophthalmologic examination revealed reactivation of herpetic epithelial keratitis while on treatment dose of 1500mg Valacyclovir TID PO. Subjectively, the patient felt significantly better. Visual acuity had improved to 20/25-2 ph in each eye.
Given recurrence of dendrites while on PO medication, he underwent another PICC line placement and course of IV Acyclovir at 750mg TID. Steroids were avoided due to an active epithelial defect in the cornea. At this recurrence, ID suspected a potentially undiagnosed autoimmune disease such as rheumatoid arthritis. This suspicion was based on the patient's age of onset, absence of HSV IgG despite ability to produce VZV antibodies, bilateral symptoms, and persistent dendrite formation after 4 weeks of IV acyclovir and 2.5 weeks of oral valacyclovir.
Ophthalmology experts in HSK at University of New Mexico were consulted who believed some of the images look like HSV, some more like VZV, and some medication-related. Overall, however, it was believed this case was infectious. The experts suspected that if not HSV, possible infectious etiologies included VZV, EBV, another human herpes virus, or an RNA virus such as enterovirus. They also suggested the possibility of a water-borne pathogen causing reinfection through shower exposure, given his immune deficiency.
Upon initiating his second trial of IV acyclovir, the patient began having clinical improvement, with decreasing photophobia, itching and erythema of both eyes. One week later he was also started on prednisolone acetate 1% in both eyes QID followed by appropriate taper. After six weeks, IV Acyclovir was discontinued, and he was switched back to oral Valacyclovir 1g TID. After completing eight weeks of PO Valacyclovir he remained asymptomatic with the right eye appearing stable without dendrites and a slight reappearance of dendritiform lesions in the left eye. His eyes overall continued to improve. At final follow-up four weeks later, his corneas were clear. At this visit, the patient recounted “I forgot how sharp some things could look...the definition and detail.” At his next follow up, he had persistent pseudodendritic lesions but no dendrites.
Allergy and Immunology ordered follow-up immunologic labs which indicated improvement in his immune function. Immunoglobulin levels returned to normal. Lymphocyte activity in response to mitogens and antigens returned to normal. Fresh NK cell activity returned to normal while IL-2 enhanced NK cell activity was just slightly below the normal range, but much improved from his prior study. Taken together, these findings indicated immune recovery following acute illness and hospitalization. However, six months after this, he attempted to wean his Valacyclovir dose and had recurrence of symptoms.
DIAGNOSIS: Bilateral Herpes Simplex Keratitis
DISCUSSION
Epidemiology
Over 50% of Americans are seropositive for HSV-1 and over 15% of sexually active Americans are seropositive for HSV-2, with HSK as a common etiology of infectious vision loss [1]. It was estimated by Farooq et al. that the global annual incidence of HSK in 2012 was 1.5 million cases with approximately 40,000 cases of new monocular vision impairment annually [2]. HSK rates vary by country and socioeconomic status, however it has been reported that up to 60% of corneal ulcers in developed countries are caused by HSV [2]. HSV epithelial keratitis specifically is estimated to have an incidence of 16.1 per 100,000 person-years [3]. HSV epithelial keratitis frequently recurs, with a landmark study showing recurrence in 49.5% of patients by 10 years after the initial episode [4].
Pathophysiology
HSK is a common and serious ophthalmic condition which has the potential to cause permanent blindness with recurrent episodes. [1] Initial HSV infection spreads via direct contact with infected lesions or secretions [5]. Primary ocular HSV infection typically presents as a blepharoconjunctivitis with or without epithelial keratitis, especially in children. [5] However, HSV ocular infection can also occur after primary HSV infection in another distribution of the trigeminal nerve. After initial inoculation with the virus, HSV travels retrograde along sensory nerves to establish dormancy in host sensory ganglia. Latent infection of the trigeminal ganglion can manifest recurrent infection in any of the three trigeminal branch distributions (ophthalmic (V1), maxillary (V2), or mandibular (V3)). Viral resurfacing is thought to be triggered by extrinsic factors including psychologic stress, increased sun exposure, hormonal changes, and contact lens wear, although this concept was not confirmed by the Herpetic Eye Disease Study [5]. HSV epithelial keratitis is typically caused by reactivation of the virus with anterograde migration of the virus from the trigeminal ganglion along V1.
Corneal epithelial infection causes punctate epithelial keratitis which coalesces into branching dendritic ulcers: with linear, branching lesions centrally characterized by epithelial loss with peripheral terminal bulbs. Cellular swelling, epithelial heaping, and loss of mucin are also typically present on exam [5-7]. This pattern of central cellular loss with concomitant loss of tight junctions causes staining with fluorescein and the disruption of the mucin coat at the edges causes staining with rose bengal and lissamine green [5]. Larger regions of epithelial loss can manifest as geographic ulceration, most commonly observed when steroids are started without controlling active epithelial infection. Damage to the epithelial layer of the cornea can damage the corneal nerves with ensuing hypoesthesia [6]. HSV epithelial keratitis is driven by active viral replication, unlike HSV stromal keratitis which is driven by immune response [6]. However, immunoglobulins in the tear-film and corneal stroma counteract the epithelial infection, and with immunodeficiency, infection can be more severe [7].
Signs/Symptoms
Typical symptoms of HSV include photophobia, blurry vision, eye pain, redness, increased tearing, and decreased visual acuity. [8] Physical exam may reveal punctate lesions coalescing into dendritic lesions or opacification of the cornea.[8] Hallmark signs on slit lamp exam include dendritic branching with corneal ulceration which is best visualized with fluorescein dye. Dendrites will typically have a terminal bulb, swollen borders, and intraepithelial cell infiltration. Filaments are also common, especially in this case. [8]
Our patient presented with symptoms of blurred vision, constant bilateral redness, tearing, discharge, and debilitating photophobia. On slit-lamp exam he had a geographic ulcer present in the right eye along with dendrites in his left eye.
Testing/Laboratory work-up
HSK is typically a clinical diagnosis. However, atypical lesions or existing medication use can confound accurate diagnosis. Polymerase chain reaction (PCR) and viral culture have been widely used to aid in diagnosis; however, studies have shown that PCR may lack concordance with clinical findings and that alternative testing methods may have more utility [9]. Alternative methods such as tear collection and immunofluorescence antibody assay (IFA) are increasingly being used. [8, 9] PCR is highly sensitive, detecting 29.2% more cases than viral culture in a 2006 study conducted by El-Aal et al. [10] Another study found that PCR detected 88% of cases in patients with suspected HSK yet viral culture only identified 12%. [10] Despite the high sensitivity of PCR, it has limitations in atypical presentations. [9] PCR was found to more likely detect cases of HSK in patients with typical lesions or those who have not used antiviral medications (P=0.022), whereas it was less responsive in patients with atypical lesions or those currently or previously using antiviral medications (P=0.968). [11] Because no diagnostic modality has been universally adopted, implementing a standardized protocol could enhance the accuracy and reproducibility of HSK diagnosis. [9] Our patient had two prior episodes of HSK within the year prior to presentation treated with antiviral medication and additionally had PCR obtained for his current suspected HSK episode while taking Valacyclovir 1000mg PO three times a day. Given his past and current use of antivirals, this may explain why the PCR was negative for HSV.
In addition to a negative PCR, this patient also had a negative viral culture and negative IgG HSV antibodies. There are a multitude of reasons our patient could have been seronegative. First, his negative viral culture may have been due to the test’s low sensitivity. Second, our patient was found to have an IgG deficiency during his HSK workup. An inability to generate IgG in response to infections may provide an alternate explanation to his seronegative HSV IgG yet classic clinical presentation with multiple recurrences. [12] Third, based on our patient’s lab results, he may potentially be suffering from a specific IgG subclass deficiency rather than total IgG deficiency which could explain why he was able to still generate antibodies to VZV. [12] Finally, literature suggests that using tear samples to quantify HSV IgG may not be as sensitive as serum concentrations. In a 2010 study by McBride et al. the local IgG antibody response in HSK was analyzed. [13] Using an enzyme-linked immunosorbent assay (ELISA), serum IgG levels were compared to the tear samples. [13] Researchers found that HSV specific IgG1 and IgG4 serum concentrations were 16.1 and 6.5-fold higher respectively than in tears, highlighting the decreased sensitivity of tear sample IgG compared to serum. Difficulty in obtaining sufficient tear samples and potential transudation of IgG from the serum to the inflamed eye may explain these results. [13]
Imaging
Treatment/Management/Guidelines:
Treatment of HSV epithelial keratitis may include systemic or topical treatments. Systemic treatments include acyclovir and valacyclovir. Topical treatments include acyclovir 3% ointment, trifluridine 1% ointment, and ganciclovir 0.15% gel. [1,5] For immunosuppressed patients or those with posterior segment involvement such as acute retinal necrosis (ARN) or progressive outer retinal necrosis (PORN), intravenous antivirals are recommended. [1] Subpar healing and multiple recurrences may indicate the presence of a resistant viral strain. Alternative medical therapies or debridement are typically necessary for these cases. [14,15]
A 2008 study by Duan et al. found acyclovir resistance in up to 6.4% of immunocompetent patients with HSK, suggesting that the cornea can be subjected to acyclovir resistant strains. [16] It has been suspected that this might be due to the immune privilege afforded to the cornea, providing a reactivation site that is subject to less immune system surveillance. [17]. It has also been confirmed that acyclovir resistant strains of HSV are able to establish latency in the trigeminal ganglion of immunodeficient individuals. [18]
Our patient displayed signs of a resistant HSK given his multiple recurrences and continued progression of disease while on oral antiviral therapy. It is difficult to decipher if a drug-resistant HSV strain or our patient’s immunodeficiency contributed to his prolonged recovery and difficult treatment. A 2006 study by Seppänen et. al analyzed the relationship between impaired humoral immunity and its correlation to recurring genital HSV-2 and herpetic neuralgia. [19] They found that low levels of total IgG1 and IgG3 antibodies were associated with recurrences of HSV-2 genital herpes. [19] Given that our patient was deficient in IgG, potentially a similar mechanism was at play in our patient’s HSV-1 HSK. If so, this could explain his multiple recurrences of HSK and subsequent case of bilateral HSK despite following standard treatment guidelines.
Furthermore, a 1989 case report identified six cases of recurrent HSK occurring in Acquired Immune Deficiency Syndrome (AIDS) patients. They found that each patient had one to three recurrences over a mean observation period of 17 months with a moderately prolonged clinical course and median healing time of 3 weeks using topical antiviral treatment. The median dendrite-free interval was found to be 7 months. [20] Additionally, studies have shown that it is possible, albeit rarely, for a simultaneous VZV/HSV co-infection in immunocompetent patients, highlighting the role of one’s immune system in protecting against these viral infections. [21-23] These cases shine light on the delicate interplay of immunodeficiency on HSK recurrence, course, and recovery.
This case was challenging because the patient responded to IV but not oral antivirals, suggesting possible decreased gastrointestinal absorption. Given his past medical history of asthma and eczema as a child along with present-day allergic rhinitis, his mucosal changes may be related to atopy or a subsequent autoimmune process affecting PO medication absorption. Furthermore, his IgG deficiency and potentially specific subclass deficiency complicate the clinical picture, making it difficult for standard treatments to be effective.
Despite the ambiguity as to why our patient failed initial standard treatment for HSK, he began to recover with IV acyclovir and improved both symptomatically and objectively on slit-lamp exam. This case highlights the complexity of treating HSK in patients with underlying immunodeficiencies and atypical presentations. It underscores the importance of considering alternative diagnoses and treatment strategies when standard care does not yield expected results. Collaborative efforts with specialists are crucial in managing such complex cases effectively. This case highlights the importance of individualized care and consideration of novel pathogens, resistance, or immune deficiency in recurrent infections.
EPIDEMIOLOGY/ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Related Case: Interstitial keratitis secondary to Herpes Simplex Virus (HSV)
Related Case: Herpes Simplex Keratitis
Davis K, Hunt M, Matharu KS. Bilateral HSV Keratitis Refractory to Treatment. EyeRounds.org. August 29, 2025. Available from https://EyeRounds.org/cases/372-bilateral-HSV-keratitis.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links