Prematurity and low birth weight
A 770-gram male infant was born at 25 weeks gestational age and was admitted to the neonatal intensive care unit (NICU). His hospital course was complicated by bronchopulmonary dysplasia, patent ductus arteriosus, feeding difficulties, and apnea. Due to his prematurity and low birth weight, pediatric ophthalmology was consulted when the infant's post-conceptual age was 31 weeks to screen for retinopathy of prematurity (ROP).
None
Non-contributory
Non-contributory
As provided in the history of present illness
Winces to light in each eye
Unable to assess due to patient's age
Fully horizontal to doll's head maneuver
Soft to palpation in both eyes (OU)
Jet ventilator, pressures 23/7, rate 360 breaths per minute with fraction of inspired O2 (FIO2) 0.23-0.27, 97% O2 saturation
According to protocol, the patient's first retinal exams performed at a post-conceptual age of 31 weeks and 1 day. At the first screen, the patient's ROP status was Zone I-II, Stage 0; therefore, the patient was seen two weeks later. The progression of the patient's ROP over the following five months is displayed in Table 1, below. The worst ROP status was at 46 weeks post-conceptual age, at zone II, stage three, pre-plus disease in right eye (OD, Figure 1) and zone II, stage 3, plus disease in the left eye (OS, Figures 1 and 2). At this time, the decision was made to treat the avascular retina with ROP laser indirect ophthalmoscopy (LIO) photocoagulation in both eyes (OU), leading to regression over the next 2-3 months. There were no incidences of retinal detachment. He was discharged home with a nasal cannula providing 1.5 liters per minute (LPM) oxygen at a FiO2 of 1.0, which was gradually stopped at 10 months of age. He continued to follow-up with the pediatric ophthalmology team. His parents noted that he did not have crossing or drifting, and was able to look at the television 15 feet away. He has been growing and developing well since then.
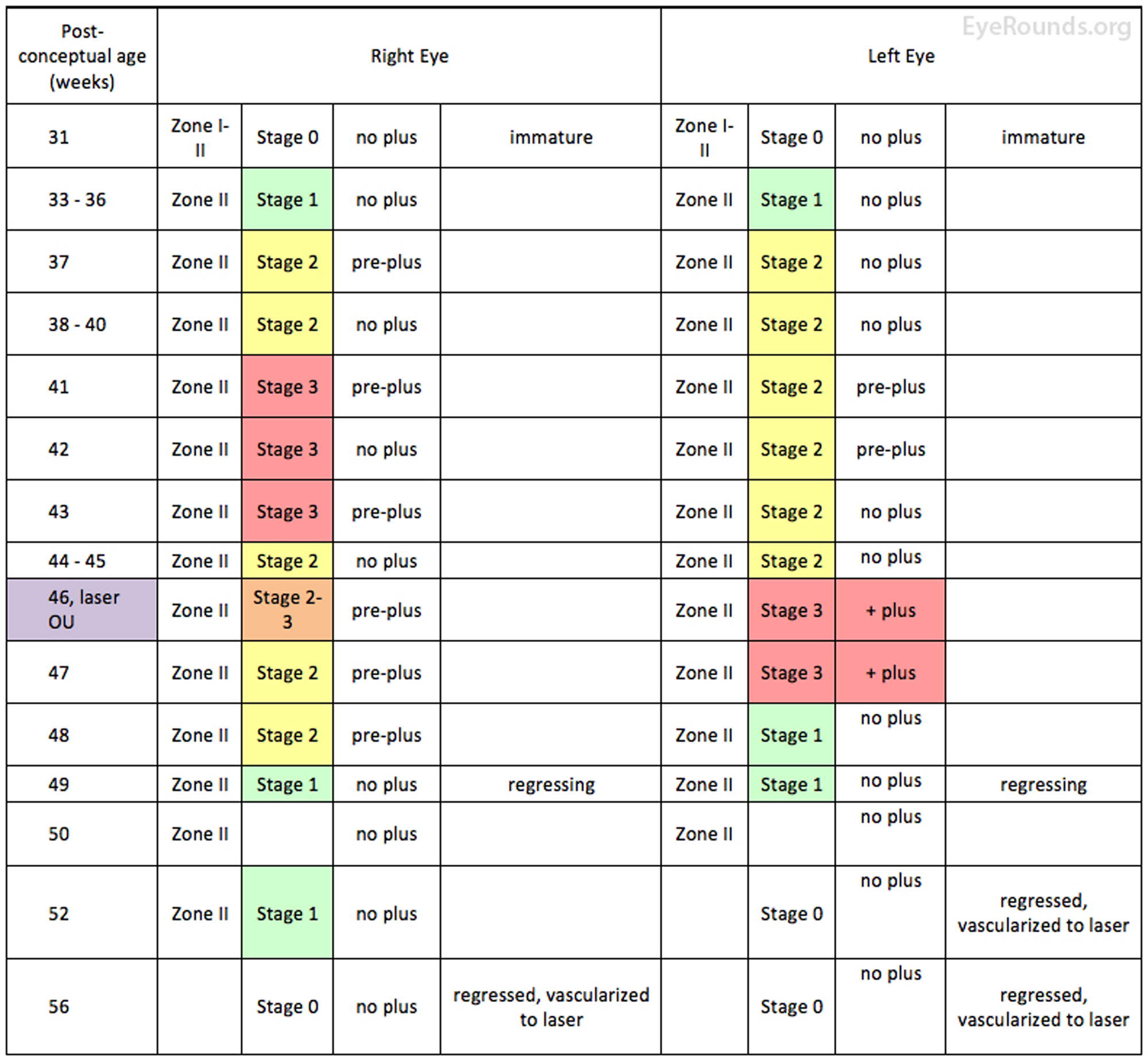
Table 1. Clinical course of premature infant showing the location, stage, and severity of ROP over time. The patient underwent LIO photocoagulation OU at post-conceptual age 46 weeks, at which time there was stage 3 ROP in zone II OU with bilateral dilatation and tortuosity of the posterior pole vessels, consistent with pre-plus OD and plus disease OS.
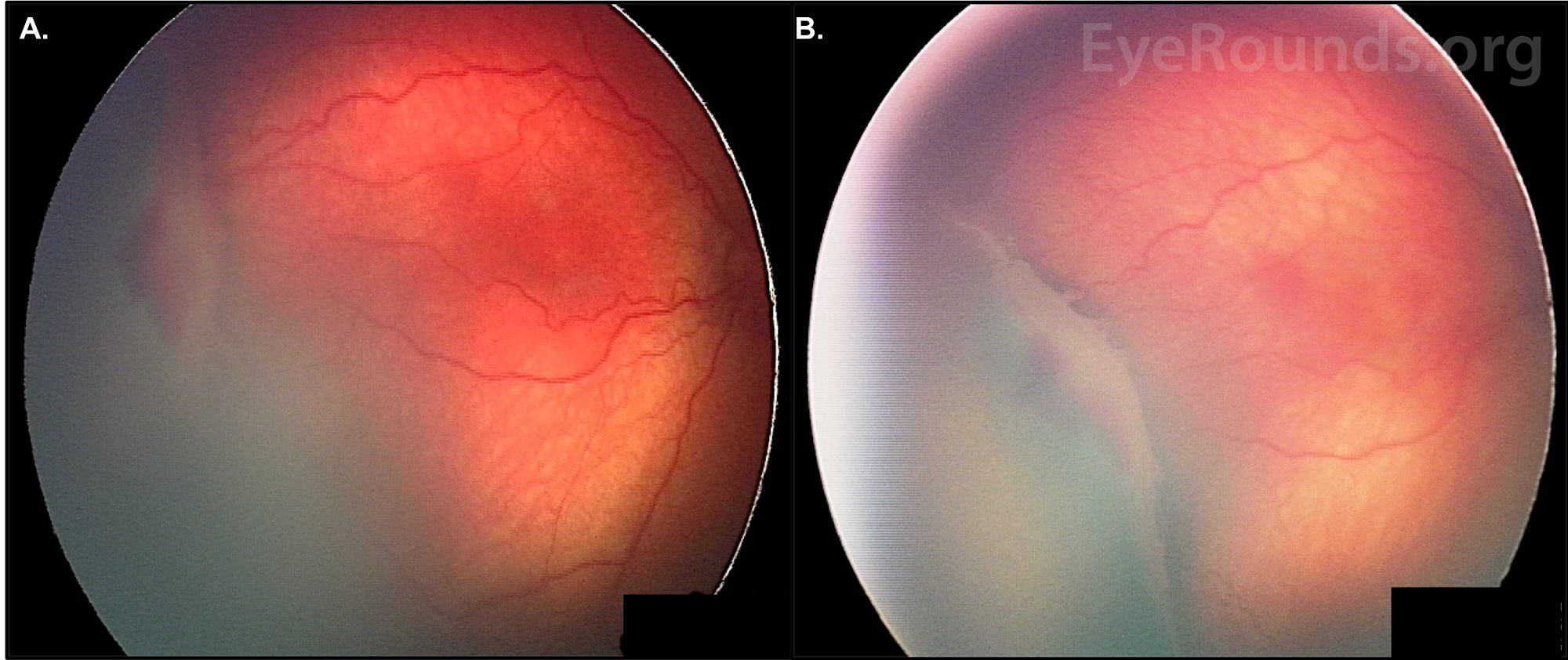
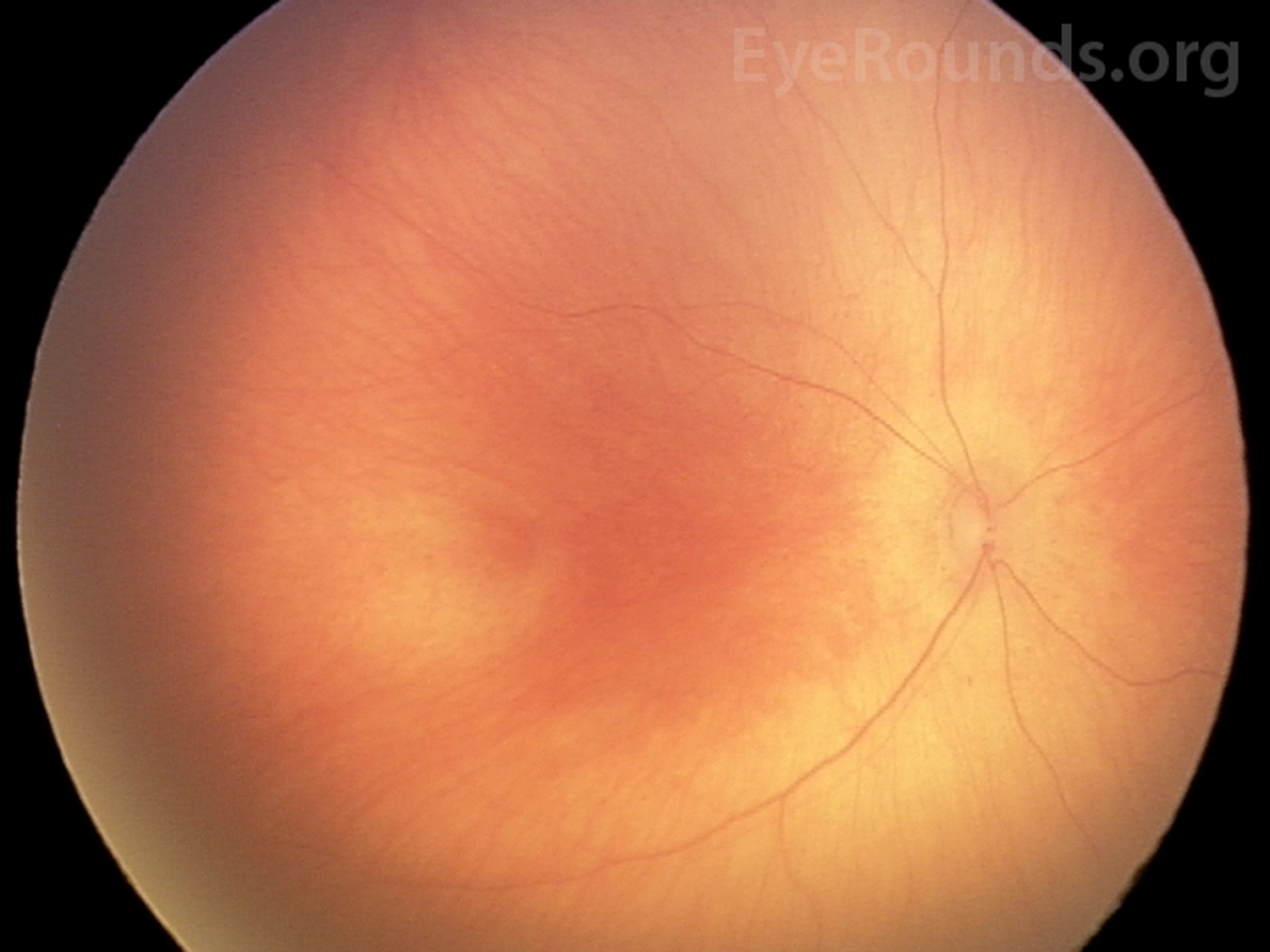
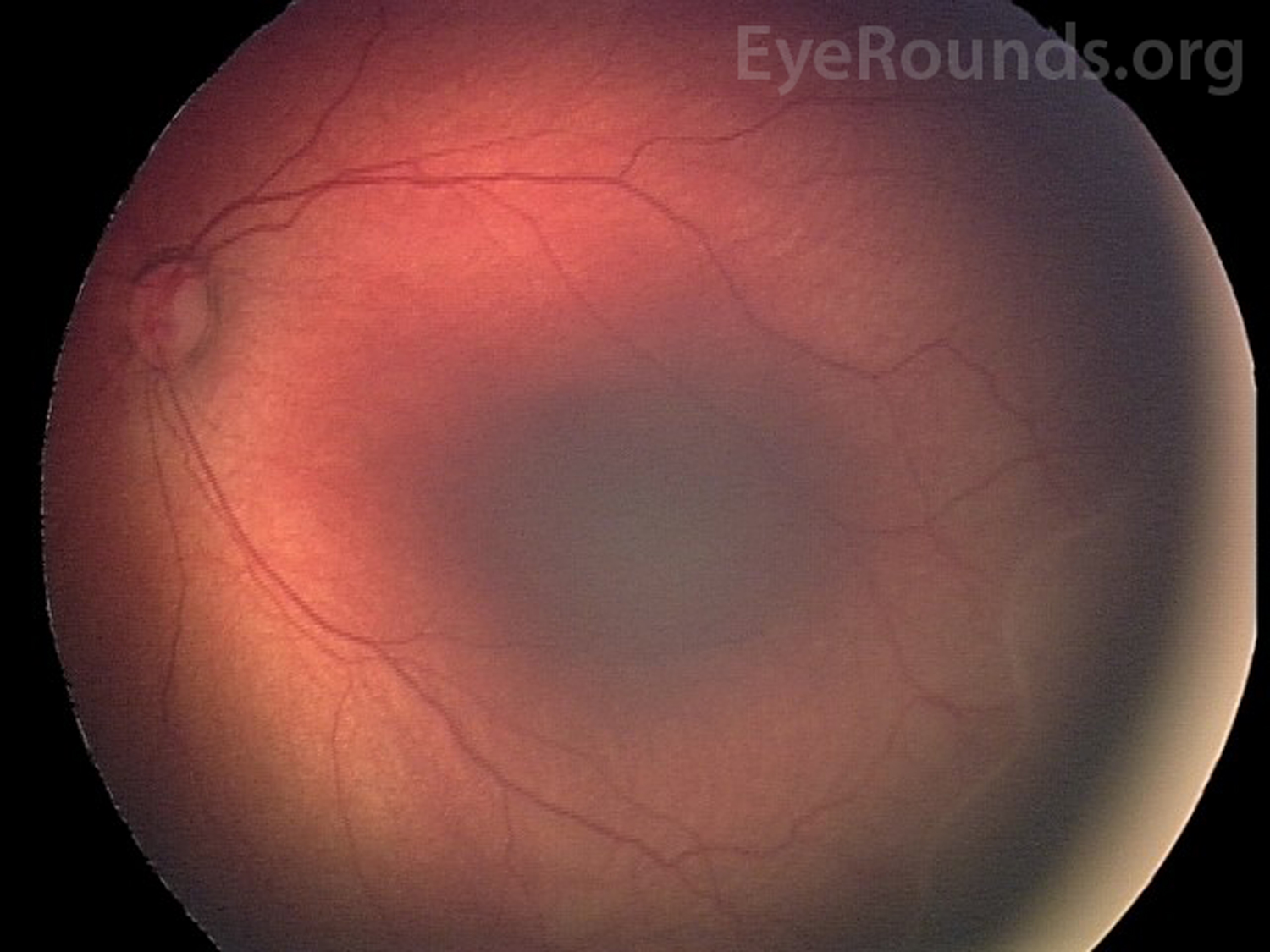
Figure 1: ROP with pre-plus disease, OD. Fundus photos of the patient taken at 46 weeks post-conceptual age. A. Stage 3 ROP is present temporally OD. A thick ridge separates the posterior vascularized retina from the avascular anterior. There is a section of hemorrhage immediately anterior to the ridge. B. A wider view of the ridge, offering a better depiction of its raised dimensions. There is fibrovascular proliferation on the posterior edge.
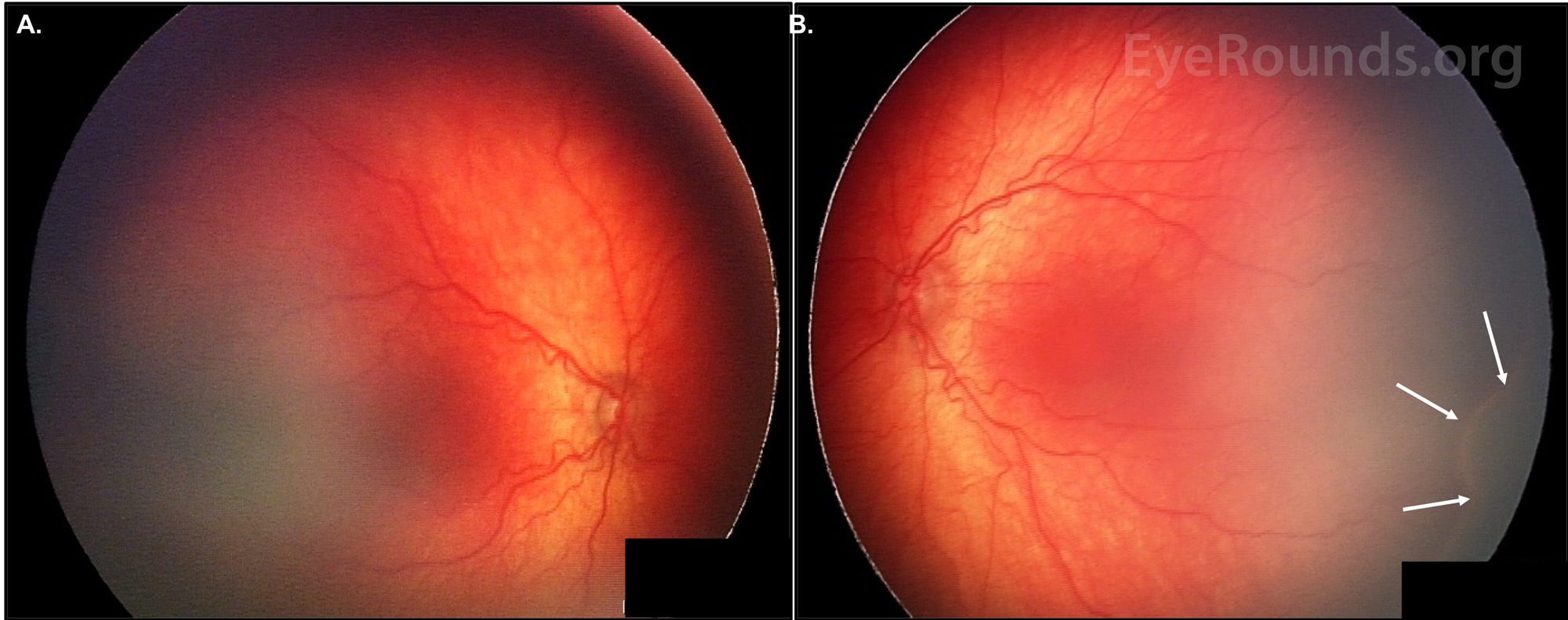
Figure 2: ROP with dilated veins and tortuous arteries in the posterior pole, OU. Fundus photos of the patient, taken at 46 weeks post-conceptual age. A. Pre-plus disease is present OD. B. Plus disease is present OS. A ridge can be seen inferotemporally (white arrows).
Retinopathy of prematurity (ROP)
ROP is the leading cause of childhood blindness worldwide. For industrialized countries, the first ROP epidemic occurred in the 1940s and 1950s. The primary risk factor for ROP in the USA and Western Europe was excessive oxygen supplementation. As a result, oxygen supplementation was harshly curtailed in the late 1950s and 1960s, leading to a decreased incidence of ROP, yet an increase in premature infant morbidity and mortality rates. The second ROP epidemic in industrialized countries began in the 1970s because of higher survival rates of extremely premature infants. The 1980s and early 1990s saw progress in ROP complication reduction and the development of new therapeutic options. The third ROP epidemic started in the early 2000s, mainly in Latin America and in Eastern Europe. These developing countries with moderate infant mortality rates (IMR) – rather than high or low IMRs – currently appear to have the highest incidence of ROP. The contributing factors in these middle-income countries include high preterm birth rates, high proportion of NICU admissions despite ongoing barriers (e.g., inadequate equipment and training, personnel shortages), and inconsistent screening and/or treatment [1, 2].
ROP continues to be a vision-threatening global issue over the past decade. In 2008, at least 50,000 children were blinded by ROP [2]. By 2010, approximately 16% of surviving infants born under 32 gestational weeks had some degree of ROP, with 3% having associated visual impairment [3]. That same meta-analysis population study revealed that 184,700 preterm babies worldwide developed ROP, of whom 20,000 became blind or severely visually impaired and 12,300 developed mild/moderate visual impairment [3]. Sixty percent of these ROP cases were thought to occur predominantly in middle-income regions of Latin America, East Asia/Pacific, and North Africa/Middle East. The Global Burden of Disease study corroborated these findings by estimating that 257,000 years lived with disability worldwide in 2010 were associated with visual impairment secondary to ROP [4]. The ROP incidence in the United States was found to have increased from 15% to 20% between 2000 and 2012, likely related to the national decline in newborn mortality rate [3, 5] at an increasingly younger gestational age. Although industrialized countries may have adopted rigorous screening and treatment guidelines that have reduced their incidences of ROP, it is probable that the worldwide incidence will increase due to increasing NICU services and infant survival rates.
Low gestational age and low birth weight are the two strongest risk factors for the development of ROP [1, 6, 7]. Both factors are associated with the extent of retinal vascular immaturity at birth and, therefore, the vulnerability to insult. The lower the birth weight and gestational age, the higher the exposure to postnatal stresses and the longer the absence of protective maternal factors [8]. This relationship has also been shown in the landmark multicenter trial, Cryotherapy for Retinopathy of Prematurity (CRYO-ROP), which includes several studies performed throughout the 1990s [9, 10]. The CRYO-ROP study found that 65.8% of infants born below 1251 grams developed some form of ROP. This increased to 90% for those born below 750 grams [10]. Despite the debate on which factor is stronger than the other, the overall literature agrees that gestational age and birthweight are both closely related to the development of ROP.
Oxygen supplementation has also been recognized as a risk factor after it's excessive use in the first ROP epidemic; however, defining the association in terms of duration and concentration of oxygen supplementation is elusive [1, 6]. Certain past studies have failed to find an association, while others have confirmed a significant association or have even shown ROP development without O2 supplementation in infants with cyanotic heart disease and anencephaly [11-14]. A study in 2001 suggested that oxygen supplementation targeting the 83-90% O2 saturation range significantly reduced ROP incidence [15]. A meta-analysis in 2017 reported that targeting O2 saturation levels below 90% decreased the incidence of ROP requiring treatment but increased the risk of death and necrotizing enterocolitis, concluding that the benefits and harms of oxygen saturation target ranges must be weighed within the local setting [16]. A 2017 study by Colaizy, et al. showed that ROP progression and active proliferation were significantly decreased after implementation of an oxygen therapy protocol [17]. Overall, these studies suggest that oxygen supplementation has a role in both ROP development and treatment. The exact management, however, continues to be unclear and remains up for debate.
Numerous other risk factors have been proposed. Some of these include low insulin-like growth factor-1 (IGF-1) levels, poor postnatal weight gain, hyperglycemia, apnea, severe illness (e.g., sepsis), blood transfusions, xanthine administration, indomethacin usage, intraventricular hemorrhage, respiratory distress syndrome, and maternal factors like poor nutrition, limited prenatal care, and bleeding [6, 8, 18-22]. Several recent meta-analyses found a protective effect of human milk on development of ROP [22]. The CRYO-ROP study also cited white race and multiple births as risk factors [23]. The proposal that hospital-associated ambient light may be a risk factor [24] was debunked by the multi-center Light Reduction in Retinopathy of Prematurity (Light-ROP) trial [25]. The risk of developing ROP was decreased in African Americans, mothers with pre-eclampsia, and infants with betamethasone administration or vitamin E therapy [1, 6].
Retinal vascular development begins at 16 weeks gestation with mesenchyme growing from the disc and reaching the ora nasally at 36 weeks gestation and temporally soon after full term birth at 40 weeks gestation. A primitive and immature capillary network lies on the posterior edge of the advancing mesenchyme. This capillary network undergoes absorption and remodeling to form mature retinal arteries and veins. The physiologic level of vascular endothelial growth factor (VEGF), necessary for normal retinal vascular development, is inversely proportional to the oxygen content.
In phase 1 of the development of ROP, hyperoxia, postnatal stressors, and lack of protective in utero factors contribute to the arrest of retinal vascular development. Because the partial pressure of oxygen (PaO2) of a fetus ranges between 22 to 24 mmHg in utero (made possible due to placental oxygen exchange), the post-natal atmospheric and ventilatory oxygen content necessary for oxygenation of the immature infant lungs may cause hyperoxia. This high oxygen content then halts retinal vessel growth by decreasing VEGF production. Prolonged hyperoxia leads to vasoconstriction and ends with vaso-obliteration, resulting in an anterior avascular zone of retina (Figure 1). This avascular retina becomes progressively ischemic over the following weeks.
The transition between phase 1 and 2 generally depends on the infant's post-menstrual age rather than the post-natal age, roughly starting at 30 weeks post-menstrual age. This may suggest an association between the programmed timing of development and the disease pathogenesis. In phase 2, the increasingly metabolically active but poorly vascularized retina begins secreting VEGF and erythropoietin. Small avascular regions produce VEGF levels close to physiologic amounts such that normal vessel growth may resume. If the region is large, however, excessive VEGF production leads to arteriovenous (AV) shunts at the border between the vascularized posterior and avascular anterior retina. Regression may occur if normal vessels can grow past the AV shunts while progression begins when nodules of endothelial proliferation arise next to the AV shunts, perforating through the internal limiting membrane to proliferate on the inner retinal surface. This neovascularization can lead to fibrovascular proliferation, scarring, tractional membranes, and retinal detachment. The high VEGF levels may also cause tortuosity and dilation of exiting posterior pole vessels, typically known as plus disease (Figure 2) [1, 8, 26].
ROP is classified according to the guidelines described by the International Classification of Retinopathy of Prematurity (ICROP) in 1984, 1987, and 2005 [27-29]. Three main parameters were considered: location, extent, and severity. The following ICROP guidelines are summarized from the 2014-2015 Basic and Clinic Science Course: Pediatric Ophthalmology and Strabismus [6], the Handbook of Pediatric Retinal Disease [1], and the 2005 ICROP guideline updates [27-29].
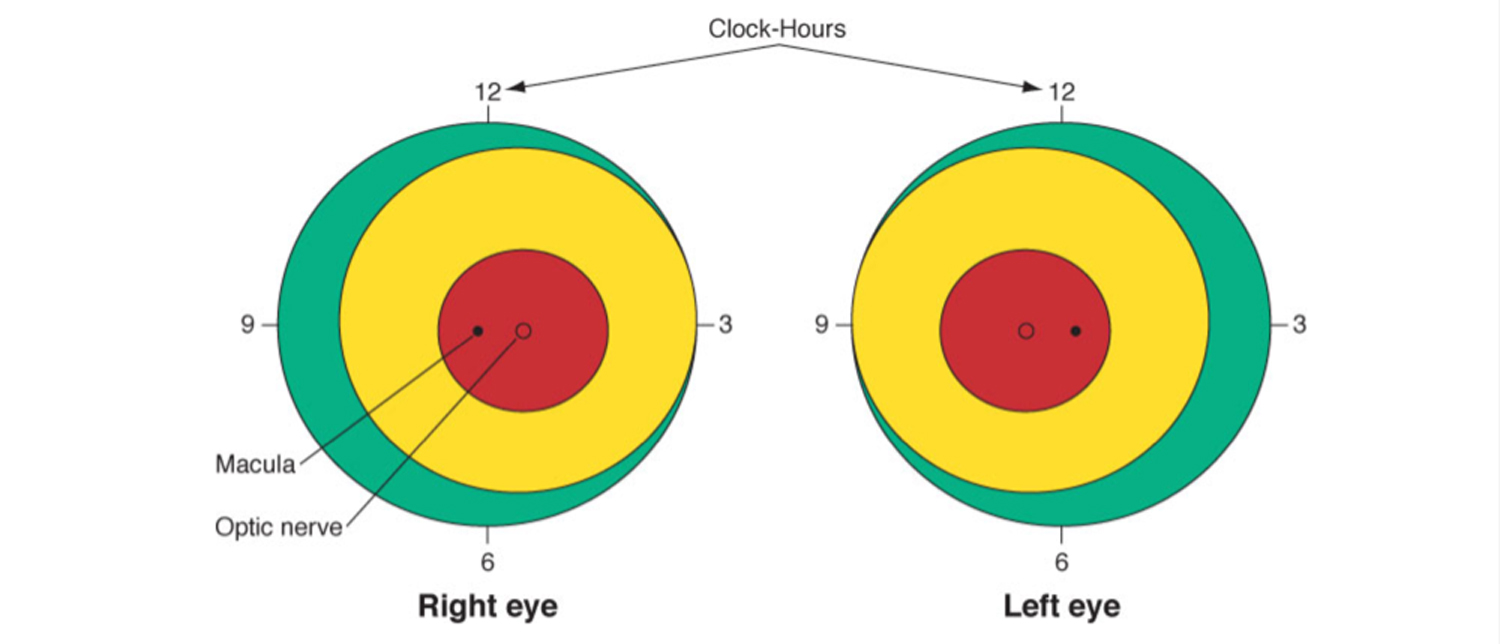
Location and Extent
| Zone I | Small circle in the posterior pole centered on the optic nerve with a radius that is twice the distance from the macula to the optic disc |
| Zone II | Extends from zone I to a tangential point on the nasal ora serrata and to the temporal equator |
| Zone III | Residual crescent anterior to zone II |
Figure 3: Depiction of zone 1 (red), zone II (yellow), and zone III (green), as well as clock-hours that describe extent of disease in ROP [6]. This figure is used with permission from the 2014-2015 Basic and Clinic Science Course: Pediatric Ophthalmology and Strabismus. |
|
Staging |
Description and Pathology |
Imaging Examples |
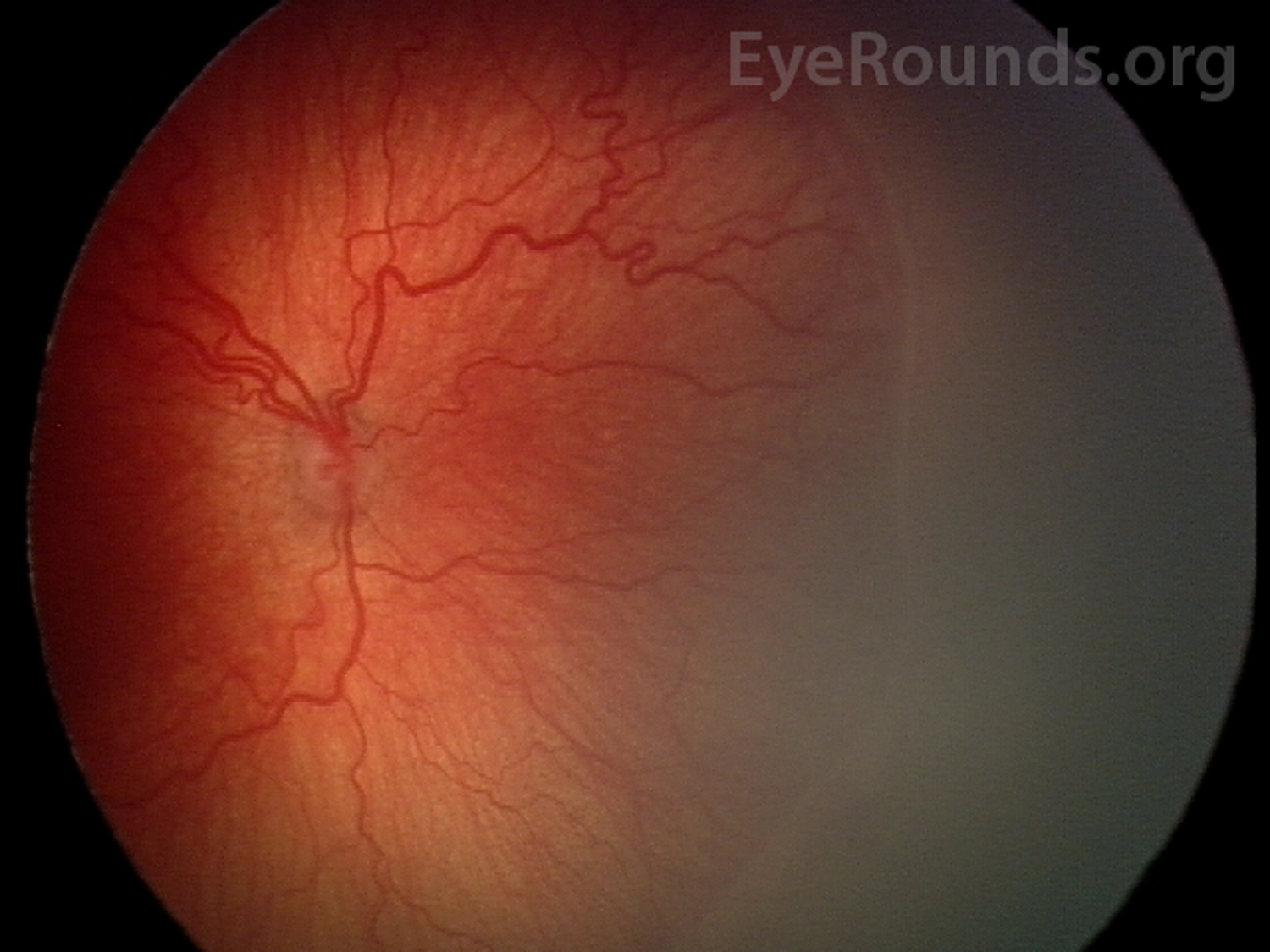
| Stage 0 | Definition: Immature vessels without ROP |
Fundus photo of stage 0 shows immature vascularization. |
| Stage 1 | Definition: Thin white demarcation line between vascular and avascular retina Pathology: Spindle-shaped cells, which are the precursors of vascular endothelium, compose the anterior part of the line. Differentiated endothelial cells of mesenchymal origin form a capillary meshwork making the posterior aspect of the line [1]. |
Fundus photo of stage 1 shows thin demarcation line (white arrows) that lacks dimensions and separates vascular retina from the avascular anterior. |
| Stage 2 | Definition: Ridge +/- posterior fibrovascular tufts Pathology: The demarcation line develops dimension due to both spindle-cell (anterior ridge) and endothelial cell (posterior ridge) proliferation [1]. |
Fundus photo of stage 2 reveals a thickened ridge with dimension. There is vascular arcading of the retinal vessels immediately posterior to the ridge. |
| Stage 3 | Definition: Ridge with extraretinal fibrovascular proliferation
Pathology: The ridge develops extraretinal fibrovascular proliferation that extends into the vitreous and appears velvety, frayed, or ragged. The placoid form is the most common compared to pedunculated and polypoid. It has a circumferential orientation. The infiltrating neovascularization is derived from proliferating endothelial cells. The vitreous humor also undergoes synchysis and condensation caused by lytic substances and depolymerization, respectively. The overall stage is determined by the individual clock hour with the worse stage [1]. |
Fundus photo of stage 3 depicts a ridge with fibrovascular proliferation. |
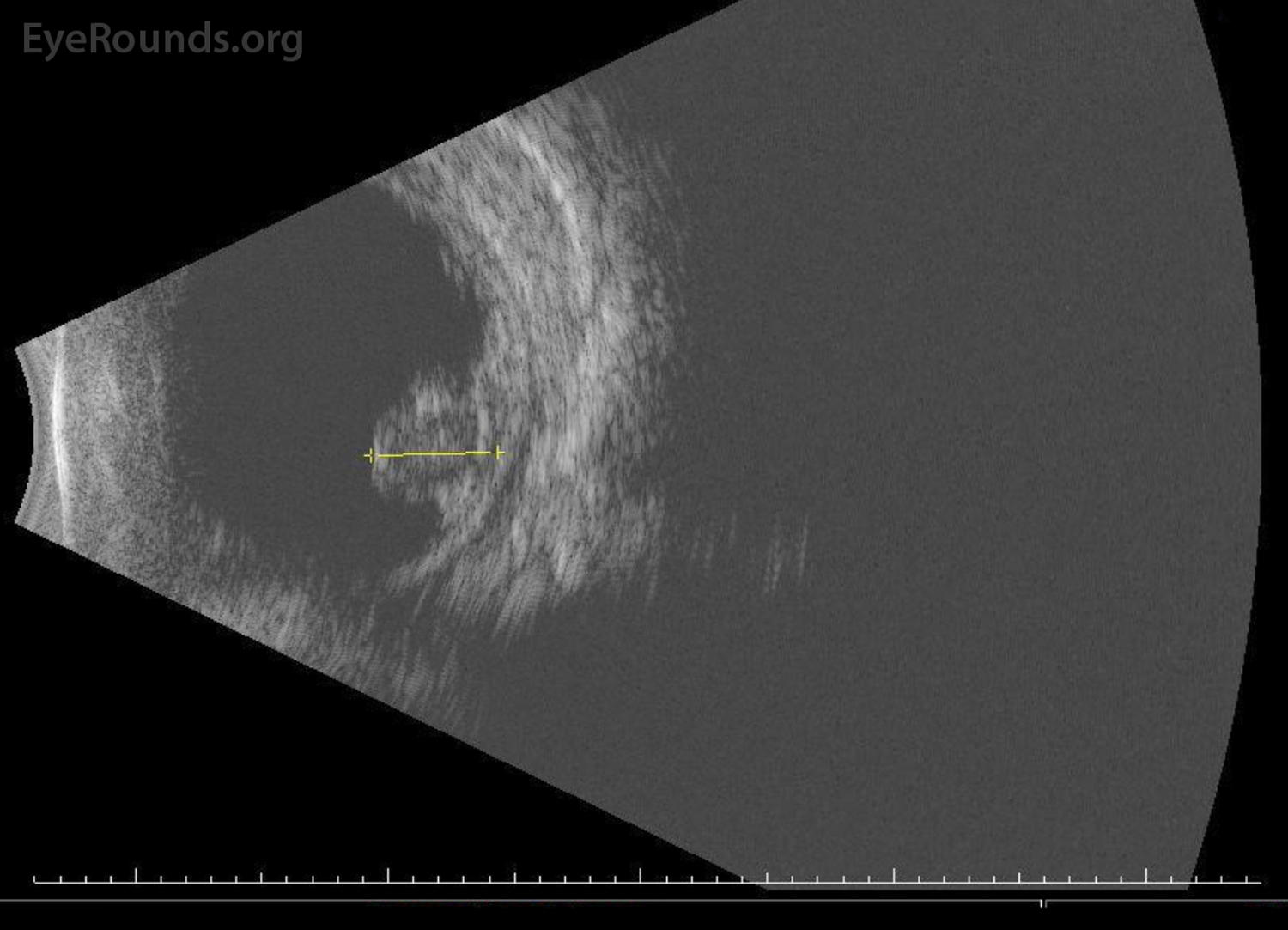
| Stage 4 | Definition: Sub-total retinal detachment
|
B-scan of a retinal detachment in stage 4 ROP. |
| Stage 5 | Definition: Total retinal detachment Sub-divided based on anterior and posterior funnel configuration:
|
Fundus photo of a stage 5 retinal detachment with open anterior and open posterior funnel regions. Used with permission from the International Classification of Retinopathy of Prematurity Revisited, 2005 [29].
Fundus photo of a stage 5 retinal detachment with open anterior and closed posterior funnel regions. Used with permission from the International Classification of Retinopathy of Prematurity Revisited, 2005 [29]. |
| Plus Disease | Definition: Dilated veins and tortuous arteries in posterior pole
|
Fundus photo of plus disease showing tortuous arteries and dilated veins. |
| Aggressive Posterior (AP) ROP | Definition: Ill-defined and rapidly progressive ROP predominantly in the posterior region with marked plus disease Pathology: AP-ROP is most commonly located in zone I. The posterior pole vessels become rapidly dilated and tortuous out of proportion to the peripheral retinopathy. Shunting occurs not only at the junction between vascularized and avascular retina but also within the retina. Hemorrhages may also be present at this junction [29]. *Previously known as Rush Disease |
Fundus photo of aggressive posterior ROP showing disease in the posterior location, prominence of plus disease, and proliferative retinopathy (arrows). Used with permission from the International Classification of Retinopathy of Prematurity Revisited, 2005 [29]. |
Table 2. Staging of ROP.
Threshold and type
The CRYO-ROP study defined threshold ROP as five or more contiguous or eight total clock-hours of stage three in zone I or II in the presence of plus disease [31], the level at which there was a 50% reduction in adverse visual outcomes when there was intervention with laser. In an effort to further reduce vision loss, prethreshold ROP was defined as zone I with less than threshold ROP; stage 2+, stage 3, or stage 3+ with less than required clock-hours of involvement in zone II [1, 30].
The Multicenter Study of Early Treatment for Retinopathy of Prematurity (ET-ROP) trial further classified ROP into type 1 and type 2 to guide the treatment of infants before the development of threshold ROP [32]. Type 1 was defined as any stage with plus disease in zone I, stage 3 without plus in zone I, and stage 2+ or 3+ in zone II, indicating the need for treatment within 48-72 hours. Type 2 was defined as stage 1 or 2 without plus in zone I and stage 3 without plus in zone II (Table 3) [32], indicating close observation with 1 week or sooner follow-up.
Threshold ROP |
Prethreshold Type 1 ROP |
Prethreshold Type 2 ROP |
Zones I or II
|
Zone I
Zone II
|
Zone I
Zone II
|
Table 3. Threshold and Prethreshold Classification of ROP as defined by the CRYO-ROP (31) and ET-ROP Studies (32).
Practically, the terminology of Threshold disease is no longer commonly used. The treatment of ROP is indicated in any eye with type 1 ROP32, defined as any eye with:
ROP screening guidelines were recommended by a joint statement from the American Academy of Pediatrics, the American Association for Pediatric Ophthalmology and Strabismus, and the American Academy of Ophthalmology in the "Screening examination of premature infants for retinopathy of prematurity" article published in 2001 [33]. The guidelines were then updated by the American Academy of Pediatrics in 2013 [34] and again in 2018 [35]; these guidelines are summarized below.
Gestational Age at birth |
Age at Initial Examination |
|
Post-Menstrual Age (Weeks) |
Chronologic (Weeks) |
|
| 22 | 31 | 9 |
| 23 | 31 | 8 |
| 24 | 31 | 7 |
| 25 | 31 | 6 |
| 26 | 31 | 5 |
| 27 | 31 | 4 |
| 28 | 32 | 4 |
| 29 | 33 | 4 |
| 30 | 34 | 4 |
| >30 with high risk factors | 4 | |
Table 4. Proposed ROP screening schedule adapted from updated 2018 guidelines (35).
Follow-up Time |
Classification |
| 1 week or less |
|
| 1 to 2 weeks |
|
| 2 weeks |
|
| 2 to 3 weeks |
|
The use of telemedicine techniques for ROP screening has become increasingly popular over the past two decades. Digital photographs of the retina taken by a RetCam are sent to a remote location for analysis by a trained professional. The photography and analysis may be performed by an ophthalmologist or a qualified non-physician. The Stanford University Network for Diagnosis of Retinopathy of Prematurity (SUNDROP) trial evaluated 1022 eyes with treatment warranted ROP using analyses from a remote ROP specialist. SUNDROP found that telemedicine had 100% sensitivity, 99.8% specificity, 93.8% positive predictive value, and 100% negative predictive value for detection of treatment warranted ROP[36]. Telemedicine correctly detected prethreshold, threshold, stage 4, or stage 5 ROP in 89% of eyes and plus disease in 95% of eyes according to an earlier study [37]. Results were also consistent amongst different readers analyzing the same photographs. The intrareader reliability for detection of low-risk pre-threshold ROP or worse was 100% for all 3 readers from a 2006 study [38]. The image quality was rated as "adequate" or "possibly adequate" for diagnosis in 93-100% of eyes [39]. Overall, these studies suggest that ROP screening using telemedicine has high accuracy, reliability, and validity. It may be a viable option to supplement indirect ophthalmoscopy, especially in situations where certain resources, like pediatric ophthalmologists, are scarce.
Cryotherapy and laser photocoagulation are the are two main types of ablative therapy for ROP. The treatment is directed at the anterior avascular retina, which produces high amounts of VEGF in ROP. Ablation of carefully selected avascular regions is thought to lower the angiogenic factor (i.e., VEGF) production, which slows neovascularization [1].
Cryotherapy can be applied transconjunctivally under topical or local anesthesia with a probe to cause ablation of the avascular regions. The CRYO-ROP study was designed to evaluate the safety and efficacy of cryotherapy for ROP. In that study, cryotherapy treatment was performed only when the ROP reached threshold status, as discussed in the Classification section above. The one-year follow-up showed that 25.7% of cryotherapy-treated eyes developed an unfavorable outcome – defined as retinal fold involving the macula, retinal detachment in zone I, or retrolental mass obscuring posterior pole – compared to 47.4% of eyes in the control group [31]. At the 10-year follow up, CRYO-ROP found that both functional (e.g., visual acuity) and structural (e.g., fundus status) outcomes were improved in the treatment group versus the control group [40]. Cryotherapy-treated eyes only had a 5% visual field reduction compared to the fellow eye [41]. Overall, the CRYO-ROP studies support the long-term efficacy and safety of cryotherapy treatment [1].
More commonly, ablation is performed by laser application using indirect ophthalmoscopy. The benefits are increased convenience, ease of administration, less need for anesthesia, and better patient tolerance [42]. The risks, however, include corneal haze, intraocular burns, choroidal hemorrhage, and cataracts [1]. A number of studies, such as the meta-analysis conducted by the Laser ROP Study group in 1994 proposed that laser treatment was as effective as cryotherapy [42, 43]. Laser-treated eyes were even found to have better structural (retinal dragging) and functional (visual acuity) outcomes compared with cryotherapy treated eyes at the 10-year follow-up after treatment [44]. The ET-ROP trial recommended early treatment of high-risk prethreshold ROP (i.e., type 1 ROP) with ablative therapy to reduce unfavorable outcomes; observation of type 2 ROP for detection of further progression was recommended [32]. Overall, these studies not only support the use of laser photocoagulation as a viable cryotherapy alternative but also encourage the early treatment of ROP with either laser or cryotherapy before progression to threshold status.
Ablative treatments, namely laser photocoagulation, may lead to permanent peripheral visual field loss, induction of myopia, intraocular burns, cataract formation, vitreous hemorrhage, strabismus, among others. Concern with these issues led to the proposal that non-destructive anti-VEGF factors, such as bevacizumab, could be used as a treatment alternative. The Bevacizumab Eliminates the Angiogenic Threat of Retinopathy of Prematurity (BEAT-ROP) study was a randomized, controlled trial that compared intravitreal bevacizumab monotherapy to conventional laser therapy for stage 3+ in zone I and II ROP [45]. BEAT-ROP found that bevacizumab therapy produced significantly better benefit for zone I, but not zone II, and allowed peripheral vessels to continue growing unlike laser-induced ablation [45]. Bevacizumab injection was also easier to administer at the bedside compared to laser treatment.
However, BEAT-ROP was not able to statistically assess bevacizumab's safety profile concerning mortality and toxicity [45]. ROP recurrence and retinal detachments have been reported after bevacizumab treatment at a later onset compared to laser treatment, raising the concern that BEAT-ROP may have not fully captured recurrence and complication data [46]. The Pediatric Eye Disease Investigator Group (PEDIG) studied various doses of bevacizumab for treatment of type I ROP; this dose de-escalation study demonstrated that a lower dose of bevacizumab (e.g., 0.031mg) may reduce the risk for neurodevelopmental disability or detrimental effects on other organs while maintaining efficacy [47]. A Cochrane meta-analysis in 2018 reviewed six clinical trials using intravitreal anti-VEGF for treatment of type I ROP; a total of 383 infants were included in the combined dataset [48]. These data showed that anti-VEGF monotherapy reduces the risk of refractive errors but does not reduce the risk of retinal detachment or recurrence of ROP. Further, this monotherapy potentially increases the risk of recurrence in zone II ROP, and the long-term systemic adverse effects of the drugs are not known [48].
The Supplemental Therapeutic Oxygen for Prethreshold Retinopathy of Prematurity (STOP-ROP) tested the hypothesis that oxygen supplementation would downregulate VEGF to cause regression of neovascularization in eyes with prethreshold ROP. STOP-ROP found that supplemental oxygen targeting O2 saturation range of 96-99% did not exacerbate prethreshold ROP but did not significantly reduce the number of infants requiring peripheral ablative therapy. The risks, however, included adverse pulmonary events, like pneumonia or exacerbations of chronic lung disease [30]. In a more recent study, biphasic oxygen targets (e.g., 85% to 92% at younger than 34 weeks and > 95% at 34 weeks and older) have shown a decrease in ROP incidence and severity without increasing mortality [49]. One University of Iowa research team published an oxygen therapy protocol, based on the STOP-ROP Trial, that has been shown to inhibit further progression of stage 2 ROP or worse in premature infants [17]. The baseline target oxygen saturations in that study were set to 85-95% and increased to >97% after diagnosis of prethreshold or worse ROP [17]. This oxygen saturation protocol is currently used at the University of Iowa Hospitals & Clinics; please see Colaizy, et al. for protocol details. There is ongoing research for development of systemic therapies (e.g., hypoxia-inducible factor stabilization) to protect the premature retina from oxygen toxicity [50].
Retinal detachments associated with late stage ROP often require surgical intervention. The surgical techniques used in advanced ROP cases include scleral buckle (SB), pars plana vitrectomy (PPV) with or without lensectomy, or a combination of SB with PPV; however, the techniques and challenges of these procedures in pediatric populations are unique. A clinician must first identify the type of retinal detachment, as ROP can cause tractional retinal detachments (most common), rhegmatogenous retinal detachments, and, rarely, exudative detachments. SB is rarely performed alone if there is preoperative proliferative vitreoretinopathy (PVR), yet one study showed that >75% of advanced stage ROP patients have PVR [51]. Thus, PPV is often the preferred surgical procedure in ROP with or without a SB. Recurrence and reoperations are increased in this cohort with approximately 38.5% of advanced stage ROP patients requiring more than one surgery [51].
A study by Gusson, et al., demonstrated long-term anatomic success in 58% of eyes undergoing PPV for ROP-related retinal detachments involving the macula [52]. However, once the macula is involved, such as in Stage 4B and Stage 5, the functional outcomes are, overall, poor even with anatomical success.
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
RISK FACTORS FOR DEVELOPING ROP [22]
|
TREATMENT/MANAGEMENT
|
Mai AP, Scruggs BA, Kemp PS. Retinopathy of Prematurity. EyeRounds.org. Posted June 24, 2019; Available from https://EyeRounds.org/cases/286-retinopathy-of-prematurity.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links