
Gradual loss of vision in both eyes with bilateral redness and irritation
A 33-year-old man from West Africa presented to the emergency department for painless progressive vision loss in the left eye for two weeks. He reported several weeks of worsening irritation and redness of both eyes. The patient also reported binocular, horizontal diplopia for the last three weeks.
On review of systems, he had intermittent chest pain and shortness of breath for the past 9 months, as well as fatigue and an unintentional weight loss of 20 pounds over the last year. His fatigue and cough had worsened over the last three weeks; his cough was productive of white sputum with no blood. He had recent night sweats, several weeks of intermittent left and right ankle swelling, and dry mouth.
He denied anorexia, mouth ulcers, fevers, nausea, or vomiting. He was previously on adalimumab (Humira) for psoriasis, but he stopped taking it approximately 6 to 8 weeks prior to presentation as he believed his worsening shortness of breath was medication-induced.
Seen two weeks prior to presentation locally for eye irritation and was given olopatadine 0.1% (Patanol®), otherwise he had no previous ocular history.
Significant for asthma, cutaneous psoriasis, gastroesophageal reflux disease, and myositis.
Adalimumab (Humira Pen) x 5-7 years, Prednisone 5mg x 7 years, albuterol sulfate (ProAir HFA) as needed for wheezing x 20 years, ranitidine 150mg orally twice daily.
The patient was a cook in a restaurant and also cleaned houses. He had no pets and no pet exposures. He never smoked and occasionally used alcohol (1 to 2 drinks per week). He was in a monogamous relationship with his wife. He immigrated to the USA in 2004, and his only recent travel was to West Africa in 2011 and 2015 for two months each trip. He denied camping or hiking.
Seasonal allergies
No known family history of eye problems, autoimmune diseases, or malignancies.

Figure 1: External photograph. On presentation, the patient had mild, bilateral proptosis, diffuse injection OU, and scattered complexion-associated melanosis OU. Patient had 20 prism diopters of exotropia with fixation of the right eye.
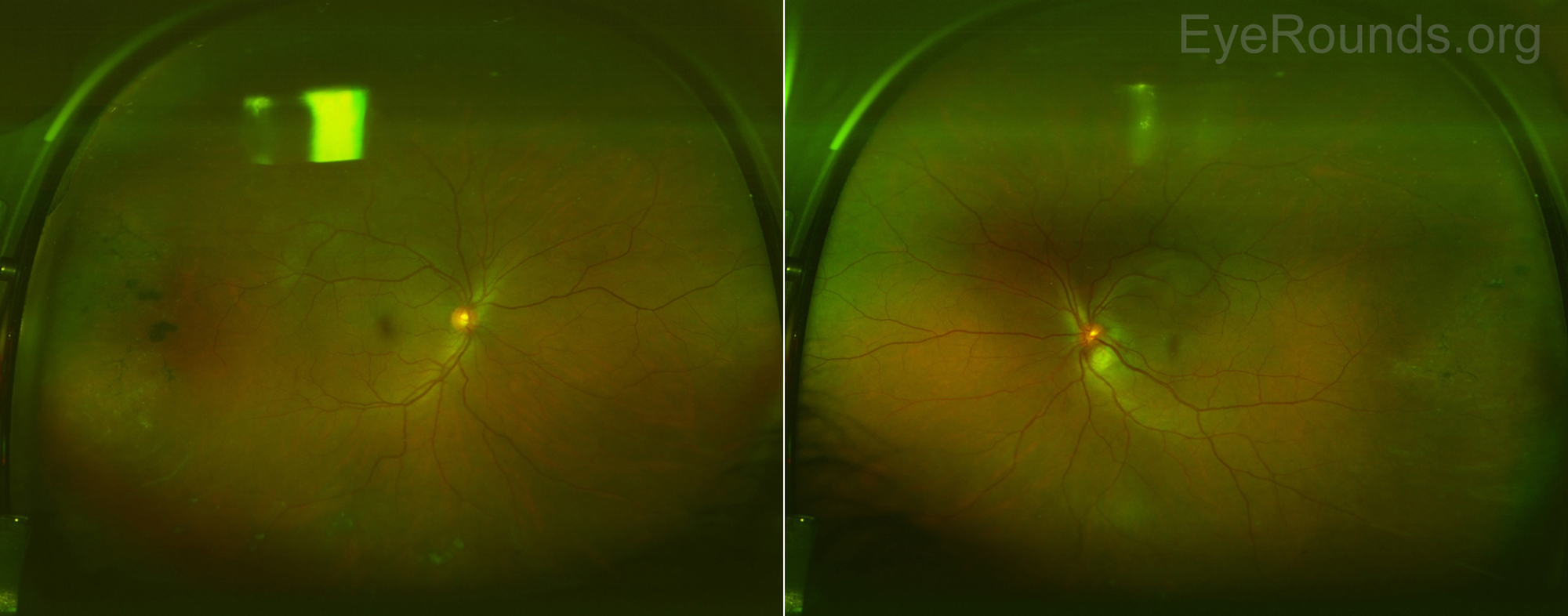
Figure 2: Optos color fundus photography. The media appeared slightly hazy in both eyes due to mild vitritis. The right optic nerve was healthy with no disc edema. There was mild disc edema of the left optic nerve and a large (~2000mm) inferotemporal retinal granuloma with surrounding subretinal fluid tracking into the macula. There were snowballs present inferiorly OU, which were difficult to appreciate in these images. There were chorioretinal scars with pigment temporally and inferiorly OU.
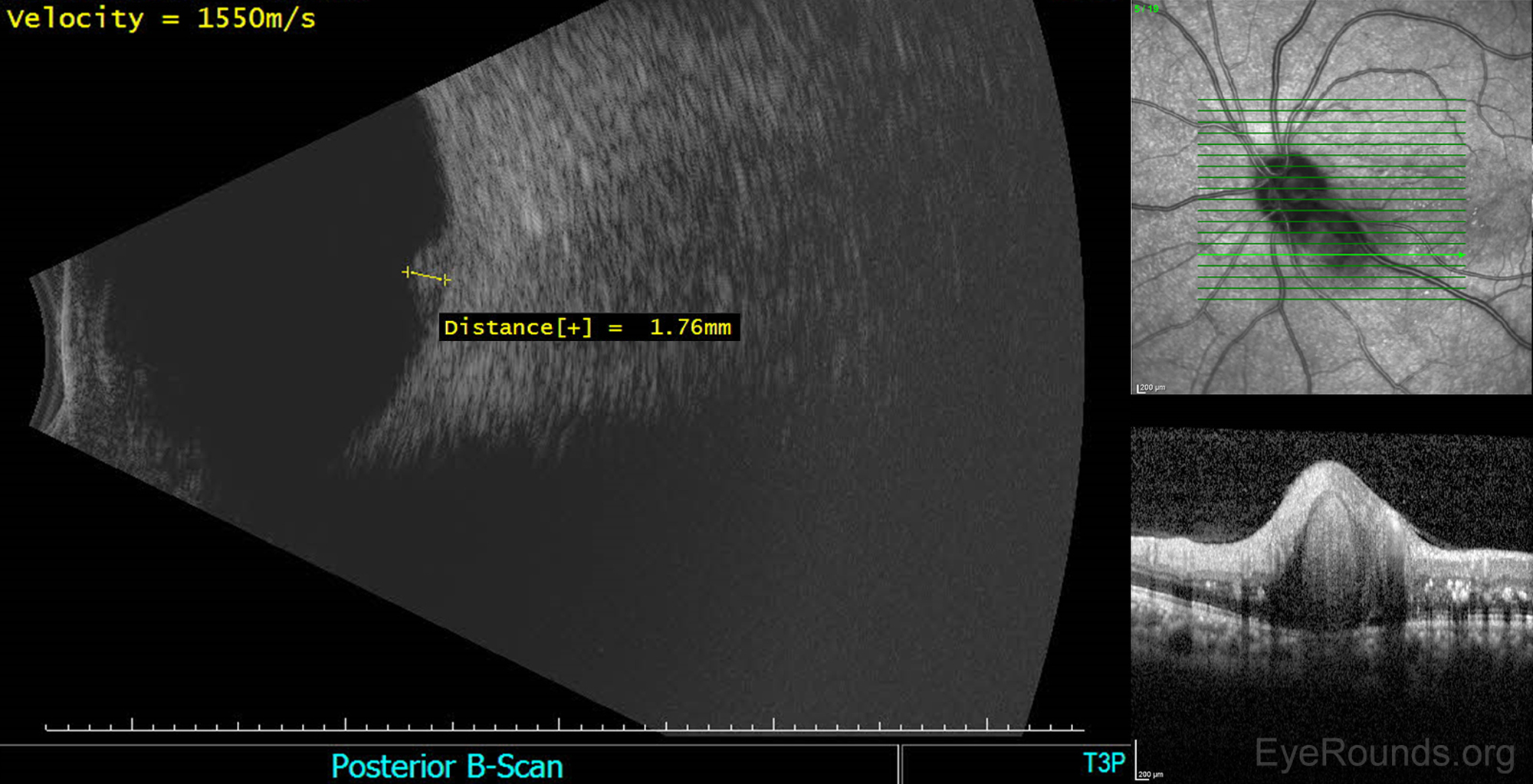
Figure 3: Echography of the left eye. Mild to moderate vitreous opacities. Just temporal to the optic disc (peripapillary), there was an elevated, high reflective lesion in the outer retina. Maximum elevation was 1.7mm. There was no retinochoroidal layer thickening elsewhere or retinal detachment detected.
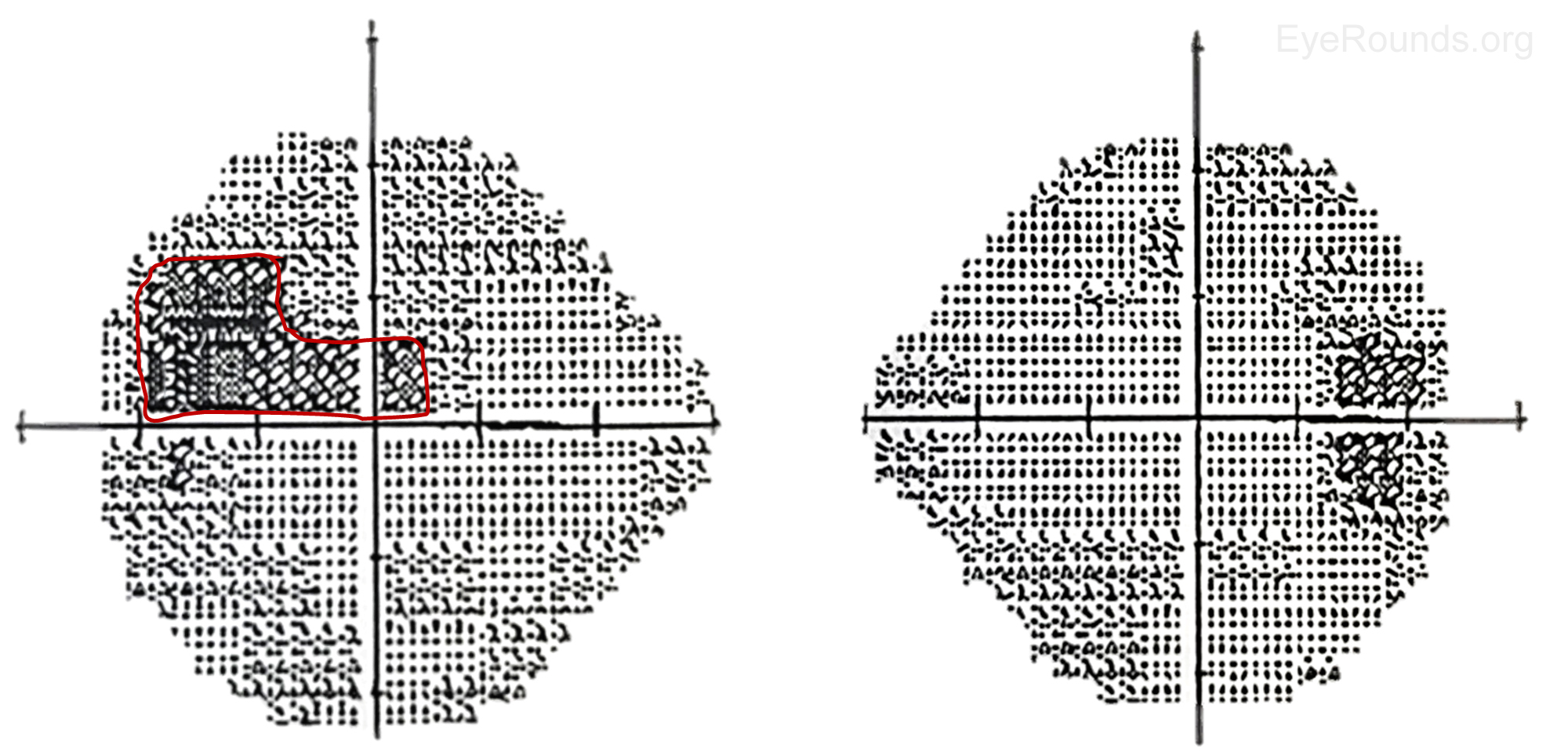
Figure 4: Humphrey Visual Fields 24-2, OU. Right eye- Several inferior and superior nonspecific visual defects, although test reliability was only fair due to 4 out of 11 fixation losses; Mean deviation -6.12dB, Pattern standard deviation 1.75dB. Left eye- Superior field deficit (red) with extension into the central field consistent with optic nerve head swelling inferiorly and subretinal fluid that extended into the macula; Mean deviation -7.88dB, Pattern standard deviation 3.73dB.
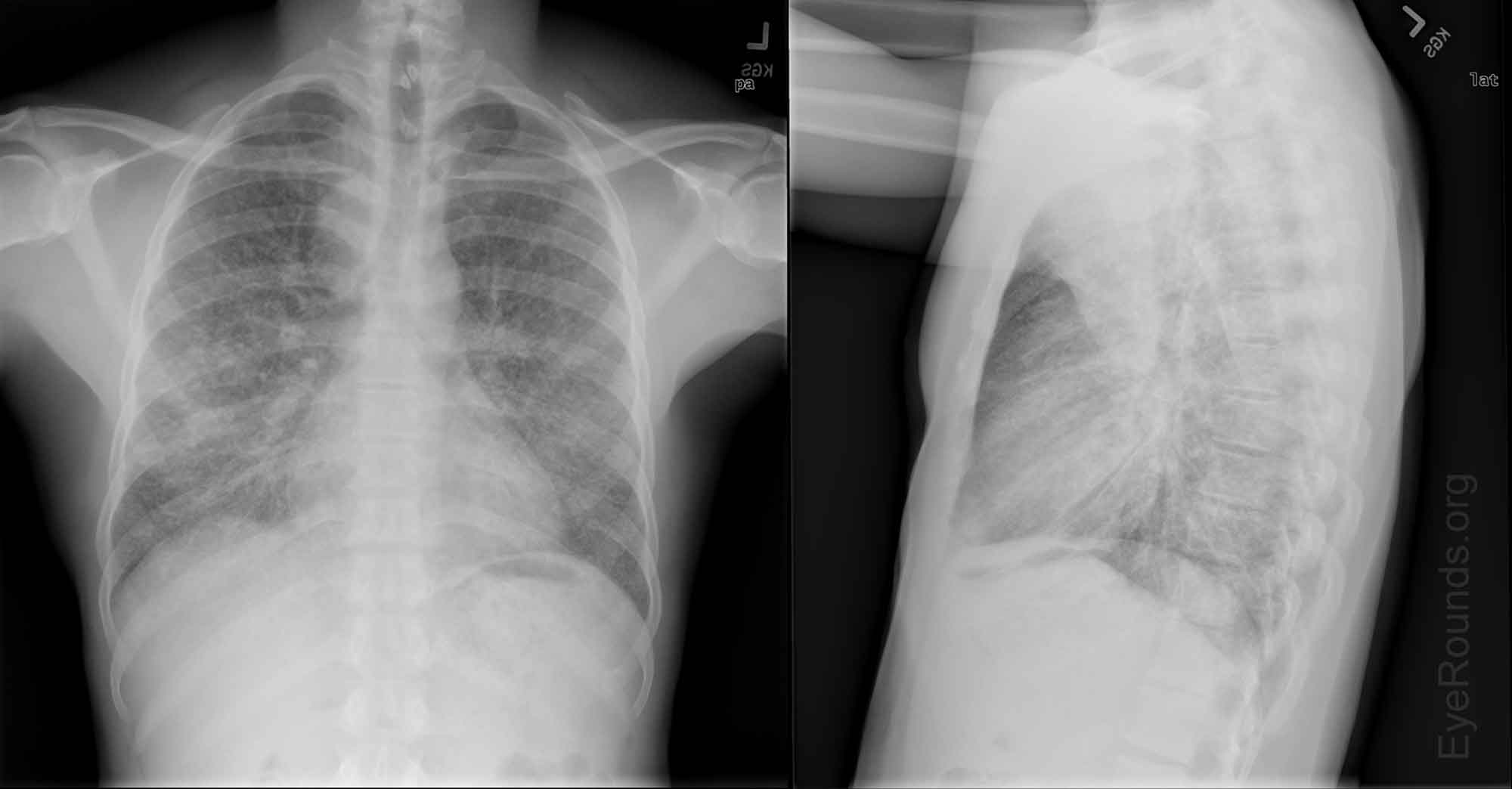
Figure 5: Chest X-ray. Diffuse interstitial and ground-glass changes throughout both lung fields which appeared symmetric and widely distributed. No evidence of associated cavitation. No parapneumonic pleural effusions. There was evidence of paratracheal lymphadenopathy.
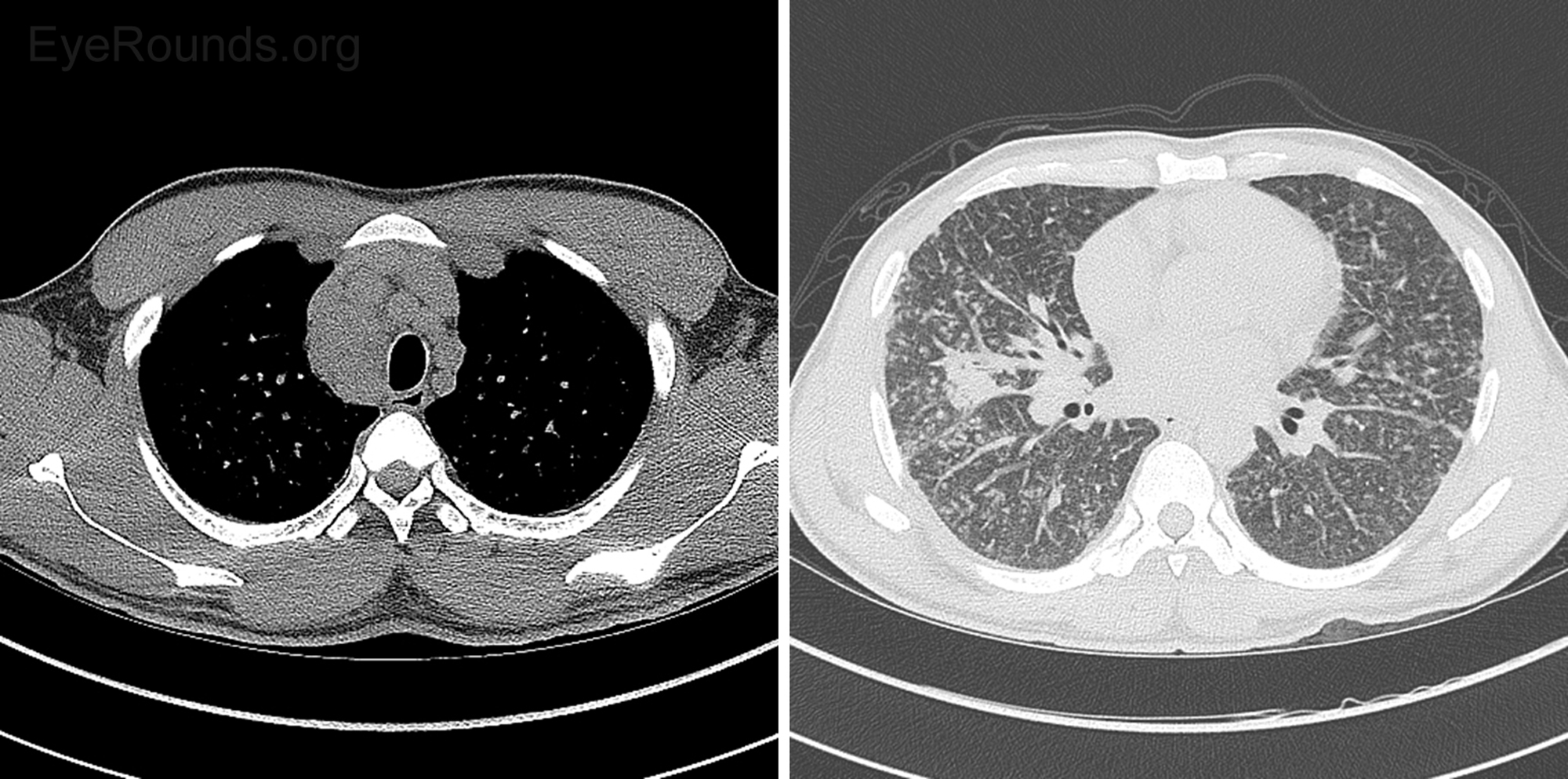
Figure 6: CT Chest without contrast. Diffuse lymphadenopathy was present and nonspecific, but given the diffuse nature was most consistent with systemic disease such as sarcoid or lymphoma. Diffuse prominence of bronchovascular interstitium with associated nodularity was nonspecific. More focal consolidation in the right middle lobe, tree-in-bud nodularity in the inferior right upper lobe, and centrilobular ground-glass nodules suggested more acute inflammatory bronchial process, such as bronchitis. Although a CT pattern of alveolar sarcoid can present with ground-glass opacities, the pattern the patient presented with was more typical of centrilobular bronchitis.
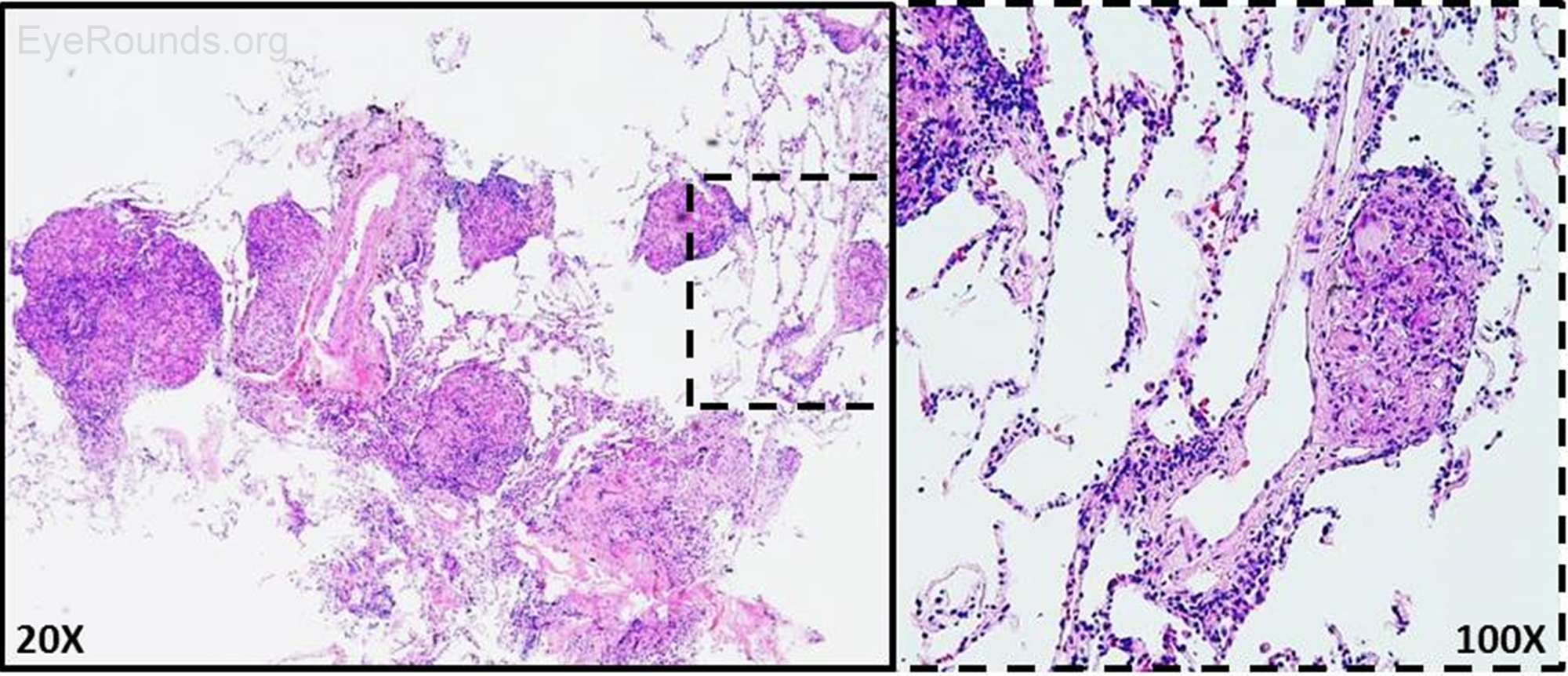
Figure 7: Right transbronchial biopsy. H&E staining of biopsied lung nodules revealed non-necrotizing granulomas. AFB and GMS stains were negative for microorganisms.
There were no intracranial abnormalities. No suspicious lesions or areas of abnormal enhancement. The optic nerves were normal bilaterally. The extraocular muscles, globes, and orbits appeared normal. The cavernous sinuses and superior ophthalmic veins were normal. There was normal signal intensity in the visualized portions of the paranasal sinuses.
On initial presentation, the patient was admitted to the medicine service for further evaluation and management. He was placed on droplet precautions given that there was a broad differential for the patient's symptoms, including tuberculosis. For the treatment of acute granulomatous panuveitis OU and disc granuloma OS, the patient was initially started on cyclopentolate two times a day OU and prednisolone four times a day OU. His intraocular pressures increased significantly over his inpatient stay with Tmax of 36mmHg OD and 35mmHg OS; thus, he was started on several aqueous suppressants OU, which were sufficient to lower the pressures below 21mmHg. Laboratory studies were remarkable for a lysozyme level of 5.82ug/mL and ACE level of 333U/L (normal: 8-52U/L). CT chest without contrast revealed diffuse adenopathy and diffuse prominence of the bronchovascular interstitium consistent with sarcoidosis. A bronchoscopy was promptly performed the following day. This confirmed the presence of non-necrotizing granulomas, and stains were negative for mycobacterium. Given his eye findings, systemic symptoms, elevated ACE level, CT chest imaging, and tissue biopsy results, sarcoidosis remained at the top of the differential. Ultimately, the patient tested negative for toxoplasmosis IgG and IgM, rheumatoid factor, ANCA, ANA, syphilis, lyme disease antibody, Histoplasma antigen, bartonella antibody, QuantiFERON-TB, PPD, HLA B27, and HIV PCR. He was discharged, and after extensive discussion between all of the specialties involved with his care, it was decided to initiate oral prednisone at 60mg per day with frequent appointments with a uveitis specialist, pulmonologist, dermatologist, and rheumatologist for management of his psoriasis and sarcoidosis.
The patient's systemic steroids were tapered slowly over several months (60mg x 1 month, 40mg x 1 month, 30mg x 1 month). He remains on 20mg of prednisone per the recommendations of the patient's pulmonologist. The optic nerve granuloma OS decreased in size significantly as shown in the color fundus photographs at presentation and after five weeks of prednisone therapy (Figure 8). Serial optical coherence tomography (OCT) images were obtained at every visit, and there was almost complete resolution of the subretinal fluid five weeks after initiating prednisone (Figure 9). The patient's vision returned to 20/20 OU within the first month of treatment, and he reported improvement of eye pain, irritation, and redness. Topical prednisolone drops were tapered slowly over two months once his intraocular inflammation resolved.

Figure 8: Color fundus photography before and after steroid treatment. On initial presentation, the patient was admitted for the treatment of acute granulomatous panuveitis OU and disc granuloma OS (Panel A). Oral prednisone was initiated at 60mg per day. The patient's systemic steroids were tapered slowly over several months (60mg x 1 month, 40mg x 1 month, 30mg x 1 month). The optic nerve granuloma OS decreased in size after five weeks of prednisone therapy (Panel B). At the follow-up visit, macular exudates were present in the left eye as a result of prior long-standing subretinal fluid OS.
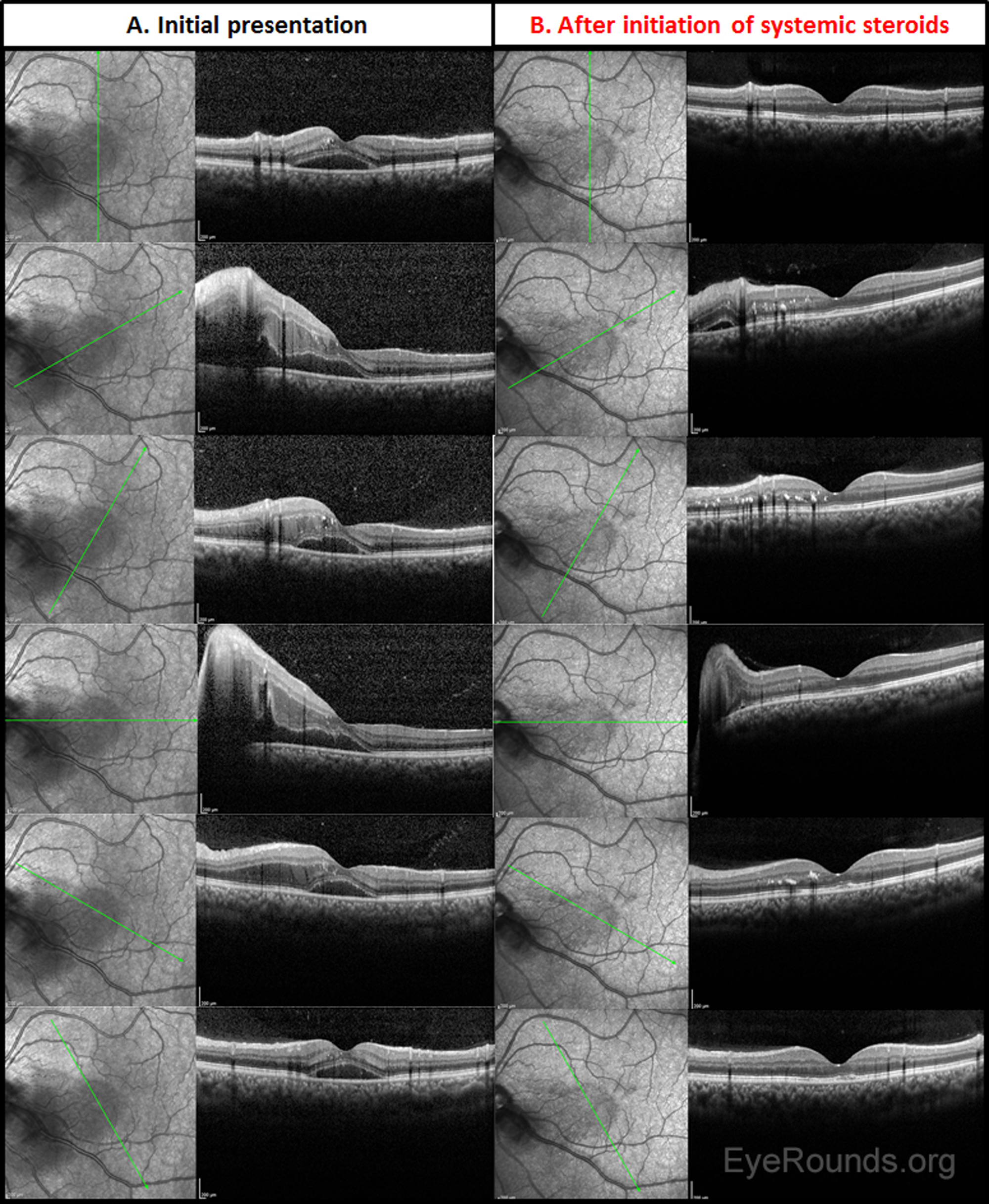
Figure 9: Serial optical coherence tomography (OCT) images. OCT images were obtained at initial presentation (Panel A) and after five weeks of prednisone therapy (Panel B). There was almost complete resolution of the subretinal fluid during this timeframe. Macular exudates were seen in the outer retina on follow-up. The patient's vision returned to 20/20 OU within the first month of treatment.
In this case, the patient had bilateral panuveitis and a unilateral optic nerve granuloma with several systemic symptoms, including weight loss, productive cough, and night sweats. Sarcoidosis is a systemic disease that is characterized by granulomatous inflammation occurring in the lungs, thoracic lymph nodes, and/or extrathoracic organs, such as the skin or the eye(s). Sarcoidosis is thought to be related to an exaggerated response of immune cells (e.g., T cells) to a variety of environmental and/or infectious antigens [1 ,2]. Monozygotic twin studies suggest that the increased Th1 response may be in part due to genetic predisposition [3]. A large multicenter analysis of over 700 biopsy proven patients with sarcoidosis, suggested that an allelic variation at the HLA-DRB1 locus may be related to developing the disease [4]. Epidemiology data suggest that this disease predominantly affects women (female to male ratio of 8:3) and African or African American patients with a bimodal age distribution [1]. Although the lung is affected in 90% of sarcoidosis patients, several studies suggest that as many as 22% of patients develop ocular involvement either early or late in the disease course [1 ,5 ,6]. Ocular sarcoidosis is the most common extrathoracic manifestation of sarcoidosis and can involve any part of the eye [1 ,6]. The most common ophthalmic presentation is anterior granulomatous uveitis, which is defined by large mutton-fat keratic precipitates, iris or trabecular meshwork nodules, and/or choroidal granulomas [5 ,6]. Additional ocular manifestations include dry eye due to lacrimal gland inflammation, conjunctival nodules, and other uveitides, including panuveitis, posterior uveitis, or intermediate uveitis. Sarcoidosis accounts for a significant fraction of all uveitides, one study citing over 5%, and it is estimated that approximately 25% of patients with ocular sarcoidosis have posterior segment disease [5 ,7].
Interestingly, when the fundus is affected, the central nervous system is also affected in 37% of cases compared to <15% of all sarcoidosis cases [5]. For this reason, MRI imaging of the brain and orbits was performed in this patient. The facial and optic nerves are the most commonly affected cranial nerves in neurosarcoidosis, and it has been documented that this disease process can affect the optic nerve head, optic tract, and/or optic chiasm, although each is very rare [1 ,6]. In fact, approximately 1% of sarcoidosis patients have optic nerve pathology, which can be identified clinically as optic disc edema secondary to inflammation, infiltration of the nerve, papilledema, optic atrophy, and optic nerve granulomas [2 ,8]. Despite this, sarcoid granulomas rarely occur in the retina, and are the rarest documented manifestation of optic nerve pathology [1 ,5]. Optic nerve granulomas in sarcoidosis were first reported by Statton, et al., in 1964 [9]. Since then, there have been fewer than a dozen case reports published that have documented such clinical manifestations of sarcoidosis [2]. Due to this, optic nerve head involvement from sarcoidosis is often misdiagnosed, especially if systemic symptoms are not yet clinically significant [1]. Still, it is clinically important to recognize them and to evaluate the level of activity. Size of the lesion and swelling of the surrounding nerve fiber layer can indicate active disease, and recent studies have shown that choroidal thickening is highly correlated with active disease [10]. OCT analysis through the granuloma shows a thickened choroid in active disease versus outer retinal tubulations, subretinal fibrosis, and loss of choroidal architecture in inactive lesions post-treatment [11].
Sarcoid involvement of the optic nerve is important to recognize and to treat promptly as such lesions may cause severe visual field defects and decreased vision. Thankfully, most of these lesions respond well to corticosteroids and/or steroid-sparing agents, such as methotrexate [1]. However, as in this case, ocular involvement is occasionally identified on the initial evaluation without a definitive diagnosis of sarcoidosis. In such cases, the differential diagnoses should remain broad, and high dose steroids are not always appropriate to start in the emergency setting. Infiltrative (e.g., lymphoma), inflammatory (e.g., sarcoid), autoimmune (e.g., HLA-B27 related diseases), vasculitis (e.g., granulomatosis with polyangiitis), and infectious disease (e.g., tuberculosis, syphilis, lyme, Bartonella, Toxocariasis, Toxoplasmosis, etc.) processes were originally considered for our patient given his clinical presentation with systemic constitutional symptoms, pulmonary findings, and panuveitis of both eyes. Fungal infections should also be considered in any patient on immunosuppressive agents (e.g., Humira).
The infectious diseases and pulmonology services were consulted due to the concern for tuberculosis and need for specialty evaluation. After much deliberation and discussion between all medical teams involved in the patient's care, it was decided to await the results of his work-up prior to starting treatment with oral prednisone, injectable corticosteroids or immunosuppressive agents. Similar to sarcoidosis, tuberculosis has a variety of ocular manifestations and should be considered when posterior pole lesions are present. Differentiation between tuberculosis and sarcoidosis can be very difficult in the early stages as both disease processes can cause infiltrative optic neuropathies, anterior or posterior uveitis, panuveitis, or retinitis. Furthermore, there are several case reports of tuberculomas occurring at the site of the optic nerve, although such a presentation is rare. In most optic nerve tuberculoma cases, prolonged duration of anti-tubercular treatment is necessary as the rate of tuberculoma resolution is usually very slow (>18 months) [12].
Cryptococcosis, toxocariasis, toxoplasmosis, lymphoma, and cytomegalovirus should also be ruled out in immunocompromised patients with optic nerve swelling [12]. Optic nerve granulomas occur in 6-19% of patients with ocular toxocariasis [13]. In fact, the optic nerve is postulated to be the entry site of the Toxocara larvae into the eye. OCT is an excellent tool for evaluation of optic nerve granulomas. In toxocariasis, these lesions often are nodular in appearance with a hyperreflective fibrotic capsule; they tend to disrupt all surrounding retinal layers while preserving the deeper optic nerve layers [13]. Conversely, OCT findings for sarcoid or TB granulomas show that they are more often located in the choroid rather than the neurosensory retina [14 ,15]. When found in the retina, TB granulomas reside in the deep retina with a hyperreflective rim and hyporeflective core representing the necrotic interior [14]). TB granulomas found in the choroid classically demonstrate the OCT findings of the "contact" sign, attachment of the RPE and overlying neurosensory retina, with surrounding subretinal fluid along with inflammatory infiltrates in the outer retina [16]. Sarcoid granulomas in the choroid are hyporeflective and homogeneous in nature [15]. One recent area of investigation is to use choroidal thickness on enhanced depth imaging OCT as a marker to differentiate between TB and sarcoid. Sattler's layer accounts for a larger proportion of choroidal thickening in sarcoidosis when compared to tuberculosis [10].
The diagnosis of sarcoidosis still remains one of exclusion and is based on clinical, radiographic, and histopathologic findings [2]. Bronchoscopy with transbronchial biopsy (Figure 7) was performed in this case due to the hilar lymphadenopathy present and markedly elevated ACE level, which indicates significant lung disease; however, there are less invasive sites that should be considered. Conjunctival biopsies should be performed if the pre-test probability for sarcoidosis is high and especially if there is a visible conjunctival lesion that resembles a granuloma. Less invasive methods of biopsies are both safer and more cost-effective for the patient while having excellent sensitivity [17]. Several studies suggest that there may be utility in performing bilateral non-directed conjunctival biopsies, although it seems that the diagnostic yield is markedly decreased compared to directed biopsies [17 ,18]. A systems-based approach to diagnosis and treatment of sarcoidosis should be followed in order to eliminate unnecessary testing.
Sarcoidosis should be on the differential for any patient with an optic nerve granuloma or in any case with vision loss associated with constitutional symptoms. For this reason, a thorough review of systems is imperative with any patient with unilateral or bilateral vision loss. Once infectious etiologies are sufficiently ruled out and the diagnosis is made, systemic steroids should be started. The route of steroid administration should be decided based on the impending threat to visual potential. In this case, our patient had 20/80 vision that improved significantly to 20/20 with high dose systemic oral prednisone, topical prednisolone, and IOP lowering agents. Had his vision been worse at presentation or had his vision declined further during the evaluation, a three-day intravenous pulse of corticosteroids would have been warranted. Several case reports suggest that intravenous methyl prednisolone can successfully treat sarcoid granulomas when initiated for several days prior to switching the patient to oral high dose prednisone (~1.0-1.5mg/Kg/day) with or without immunosuppressive therapy [1].
Although anti-TNF agents are often used to treat sarcoidosis, they are known to paradoxically cause sarcoidosis [19 ,20]. There have been over 30 case reports of adalimumab-induced sarcoidosis [19 ,20]. Our patient was informed of the risk of continuing Humira (adalimumab) for his psoriasis, and he chose to, instead, take Otezla (apremilast) for psoriasis treatment.
EPIDEMIOLOGY
|
OCULAR SIGNS
|
SYMPTOMS
|
TREATMENT
|
Scruggs BA, Ricca AM, Folk JC. Unilateral Optic Nerve Granuloma. EyeRounds.org. March 14, 2017; Available from: https://eyerounds.org/cases/248-unilateral-optic-nerve-granuloma.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
