Chief Complaint: 51-year-old female referred for consideration of cataract surgery.
History of Present Illness: Poor vision OS since childhood, and patient having more difficulty with distance vision.
PMH: hypertension, "borderline" diabetes, bipolar disorder, schizophrenia, "glaucoma".
MEDS: Seroquel, Sonata, trazodone, Lexapro, Valium, furosemide, Zaroxylyn, Travoprost.
ALLERGIES: none. FH: cataracts, arthritis, diabetes, thyroid disease.
EXAM
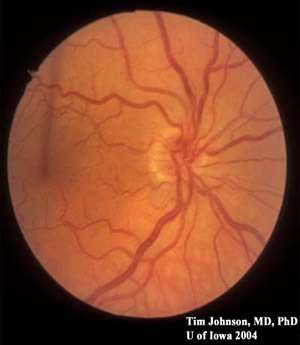
Figure 1: Stereo photos of the right optic nerve. Note the small optic nerve with crowded vessels and a pale ring around the nerve. The veins are 120-150 microns in diameter; thus, this optic nerve is less than 1 mm in diameter (average optic nerves are ~1.5 mm in diameter with ~1.2 million nerve fibers).
OD
|
OS
|
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Johnson AT: Optic Nerve Hypoplasia: 51-year-old female referred for consideration of cataract surgery. February 21, 2005; Available from: http://www.EyeRounds.org/cases/case10.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links