INITIAL PRESENTATION
Chief Complaint: Bilateral eye swelling and redness
History of Present Illness
The patient is a previously healthy, immunized 11-year-old male with no past ocular history who presents with 1 day of bilateral eye swelling and redness. Eight days prior, he developed a runny nose, cough, and temperature elevation up to 100°F. He started to feel better after four days, but on the following day his temperature was close to 100.8°F and he was coughing more. His parents alternated Tylenol and ibuprofen to manage his fever. He started to have redness and swelling of his lips and went to the emergency room two days later. His chest x-ray was concerning for pneumonia, and he was started on amoxicillin. His parents believe this was his first time taking amoxicillin. After two days, he woke up and his eyes and mouth were swollen and painful, which prompted a visit to the emergency room. His parents noticed that his eyes appeared red and that there was lots of “green goop.” He had blisters on his lips, pain with urination, and some spots on his scrotum, and so much pain in his throat that he was spitting into a bag because it hurt to swallow. He had never had symptoms like this before and denied diplopia, flashes of light, new floaters, or curtain-like vision loss. The patient was admitted for inpatient care at this time.
Past Ocular History
Past Medical History
Medications
Allergies
Family History
Social History
Review of Systems
OCULAR EXAMINATION
| OD | OS | |
|---|---|---|
| Lids/lashes | OD: Mattering of lashes with yellow crust, upper lid edema | OS: Mattering of lashes with yellow crust, upper lid edema |
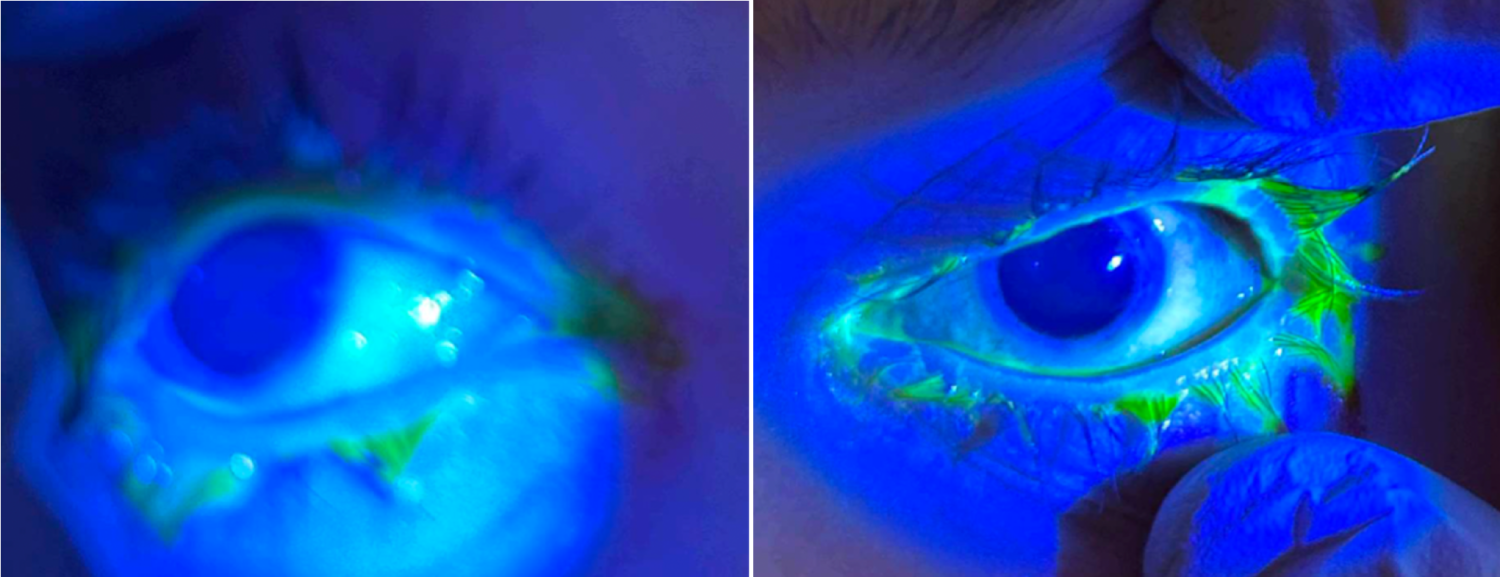
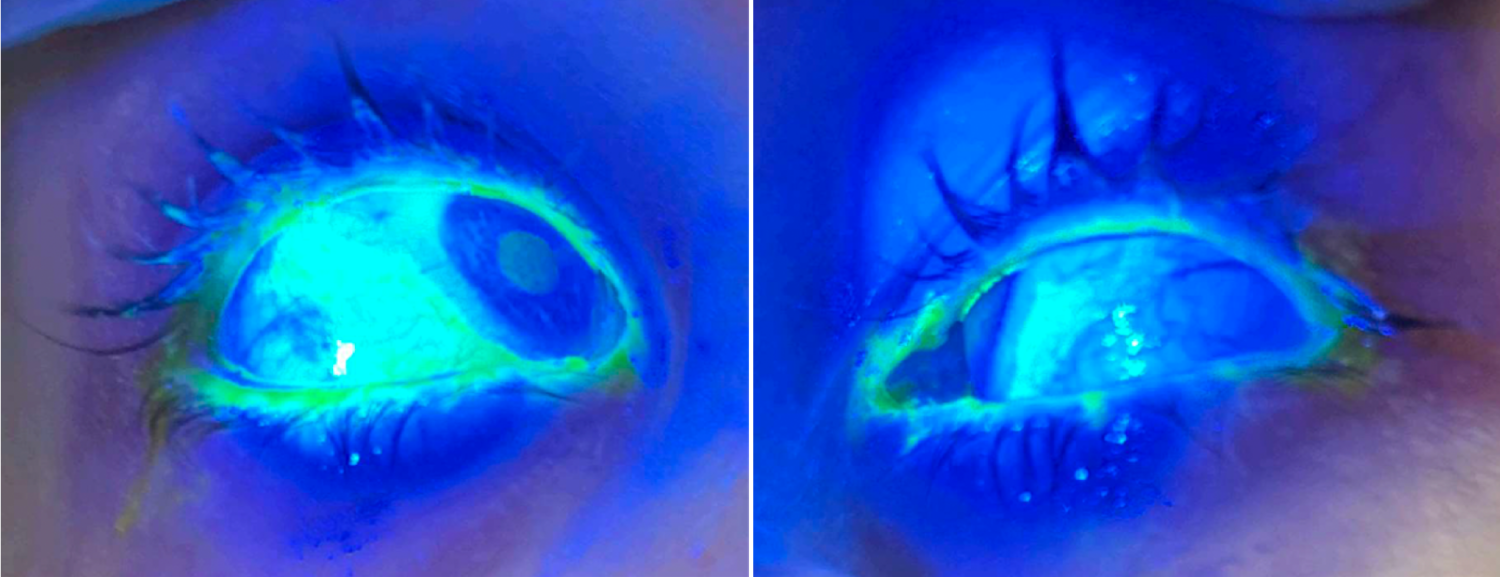
| Conjunctiva/sclera | OD: 2+ injection, inferior chemosis, bulbar conjunctival epithelial defects temporally and nasally | OS: 2+ injection chemosis, bulbar conjunctival epithelial defects temporally and nasally |
| Cornea | OD: Clear | OS: Clear |
| Anterior Chamber | OD: Deep and quiet | OS: Deep and quiet |
| Iris | OD: Normal architecture | OS: Normal architecture |
| Lens | OD: Clear | OS: Clear |
DIFFERENTIAL DIAGNOSIS:
CLINICAL COURSE
Upon admission, the patient was started on tobramycin/dexamethasone (TobraDex) drops BID to both eyes, ophthalmic lubricant ointment (Refresh PM) nightly to both eyes, and artificial tears QID to both eyes. The next day, he did not have worsening vision changes, but his conjunctival epithelial defects were enlarged compared to the exam from the day before. In both eyes, conjunctival epithelial defects were temporally and nasally enlarged, extending approximately 8mm from the limbus. In the right eye, there was a new area of injection at 8 o’clock, 7mm from the limbus. The patient was started on moxifloxacin drops QID in both eyes and prednisolone acetate 1% drops QID in both eyes. At this time, he was confirmed positive for mycoplasma IgM. Two days later, his VA remained unchanged, and injection was decreased bilaterally (+1), nasal and superior conjunctival epithelial defects were resolving, and he had stable inferotemporal defects bilaterally. The patient had 2+ punctate epithelial erosions (PEE) bilaterally. No changes to his care were made at this time. Nine days later, his exam was markedly improved; the patient’s visual acuity was unchanged, and he had mild crusting present on his lids and lashes. He had improved corneal and conjunctival involvement, with rare conjunctival injection, no membranes, good mobility of the eyelids, and no symblepharon formation. All medications were discontinued except artificial tear gel BID and he was discharged. There were no ocular concerns on follow-up 5 days later with his PCP.
DIAGNOSIS: Mucositis secondary to reactive infectious mucocutaneous eruption (RIME)
DISCUSSION
Reactive infectious mucocutaneous eruption (RIME) encompasses Mycoplasma pneumoniae-induced rash (MIRM) and is distinct from erythema multiforme (EM), Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN).(1 ,2) RIME is often triggered by Mycoplasma pneumonia infections, but there are reports of RIME secondary to Chlamydophila pneumoniae, enterovirus, SARS-CoV-2, Chlamydophila psittaci, influenza A and B, group A streptococcus, and more.(3-10) The pathophysiology is not fully elucidated but thought to be due to immune complex deposition, complement activation, and/or molecular mimicry.(2) RIME typically involves at least two mucosal sites, though recurrent episodes have been reported as limited to one mucosal site.(3 ,4) The incidence and prevalence of RIME is unclear. A systemic review by Canavan et al. reported that 94% of 202 MIRM cases presented with oral involvement, 82% with ocular involvement, and 63% with urogenital involvement.(2) The mean age of MIRM presentation was reported as 11.9 years and the mortality rate in this study was 3%.(2)
A systemic review by Haseeb et al. characterized ocular involvement in MIRM; 49.5% of cases presented with bilateral conjunctivitis and 50.5% presented with bilateral conjunctival injection or hyperemia.(11) One study reported eyelid margin staining in 86.7% (13/15) patients and purulent discharge in 77.8% (7/9) patients.(11 ,12) Four studies (6 total patients) presented corneal defects.(11) Under 10% (9/99) of patients reviewed presented with chronic ocular sequelae, including chronic distichiasis, trichiasis, lateral canthal symblepharon, scarring of eyelid margins, and more. There were no cases that presented with permanent visual loss.(11) There is a paucity of data regarding ocular presentation in RIME, which may be attributed in part to the evolution in the nomenclature to encompass MIRM.
Workup and Management
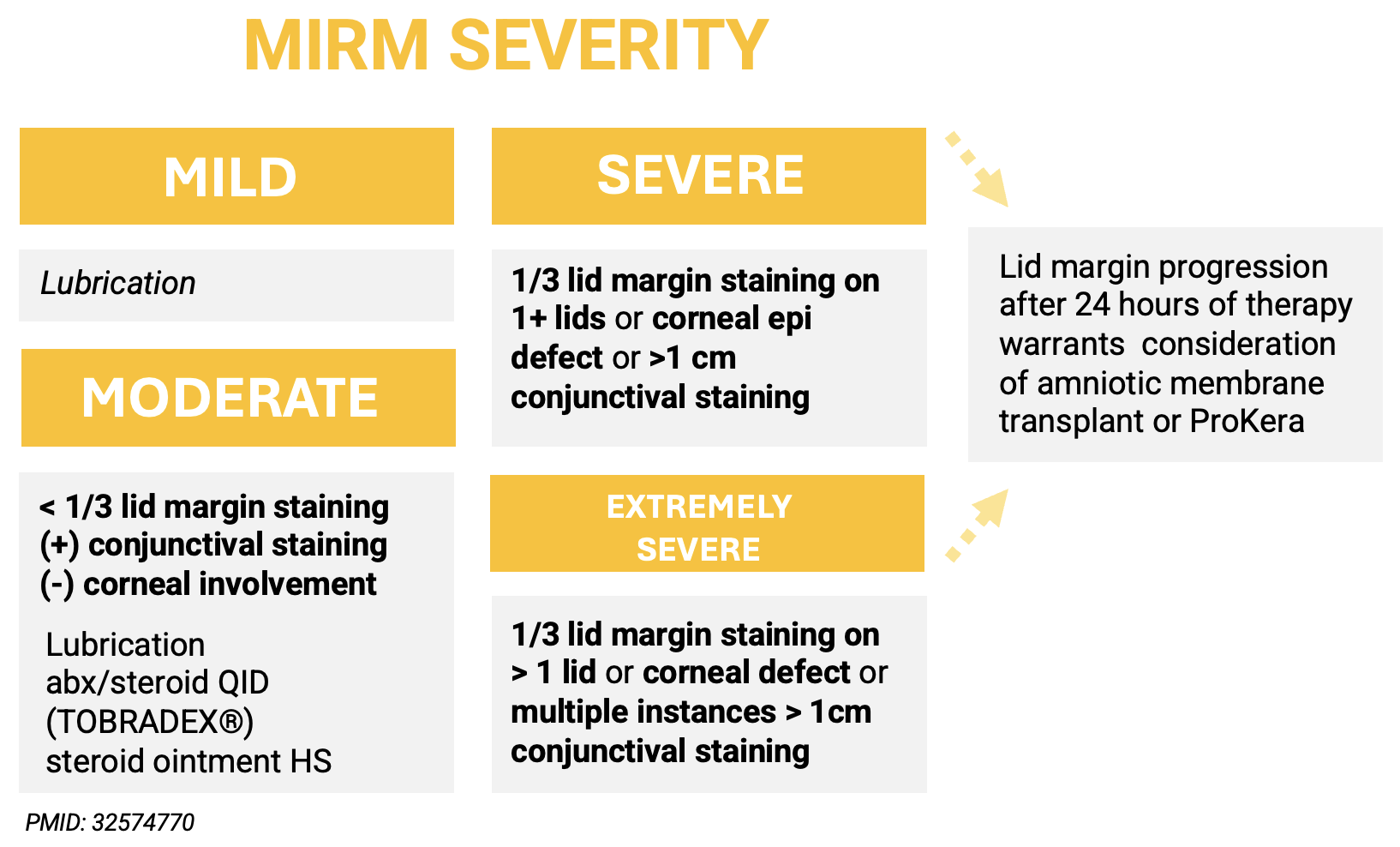
RIME treatment is largely supportive. Figure 1 depicts a MIRM treatment algorithm for ocular involvement proposed by Gise et al., which is modified from a previously published SJS algorithm by Shanbhag et al.(12 ,13)
Imaging
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
References
Sarin S, Henrie M, Dumitrescu A, Sales C. Ocular Involvement in Reactive Infectious Mucocutaneous Eruption. EyeRounds.org. May 15, 2025. Available from https://EyeRounds.org/cases/365-RIME.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links