
Sudden, painless decreased vision in the left eye
The patient is a 59-year-old woman who presented with persistently decreased vision in the left eye (OS). Her vision acutely decreased upon wakening one morning five weeks prior to presentation. She reported occasional floaters but no headache, eye pain, or eye redness. In the prior two weeks, the patient had noted "strobe lights" in the nasal aspect of the visual field OS. These photopsias worsened with coughing and quick eye movement. She had no visual changes or symptoms in the right eye (OD).
|
OD |
OS |
Visual Acuity |
20/70+2 |
20/200 |
Visual Acuity |
20/25+1 |
20/60-1 |
Intraocular Pressure |
17 mmHg |
14 mmHg |
Pupil Examination |
Reactive to light |
Reactive to light |
Motility |
Full |
Full |
External Examination |
Normal |
Normal |
Slit-lamp Examination |
Lids/Lashes: Normal |
Lids/Lashes: Normal |
Fundus Examination |
Disc: Normal |
Disc: Normal |
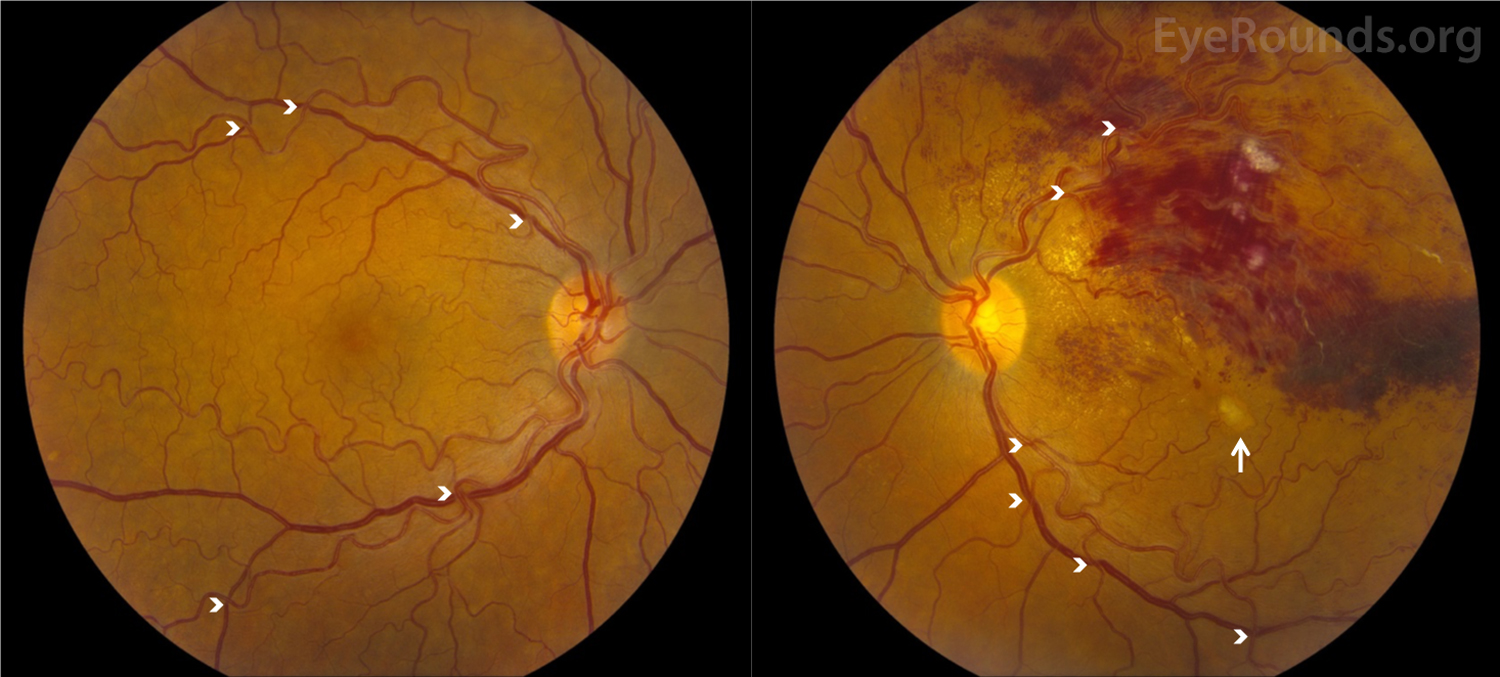
Figure 1. Color fundus photography, OU: There was marked vascular tortuosity with AV nicking OU (arrowheads). There was a recurrent BRVO along the superior arcade with massive intraretinal and retinal nerve fiber layer hemorrhages OS. There were hard exudates throughout the superior macula with a few, scattered cotton wool spots OS. There was a central macular hypopigmented lesion with a small amount of subretinal fluid OS (arrow).
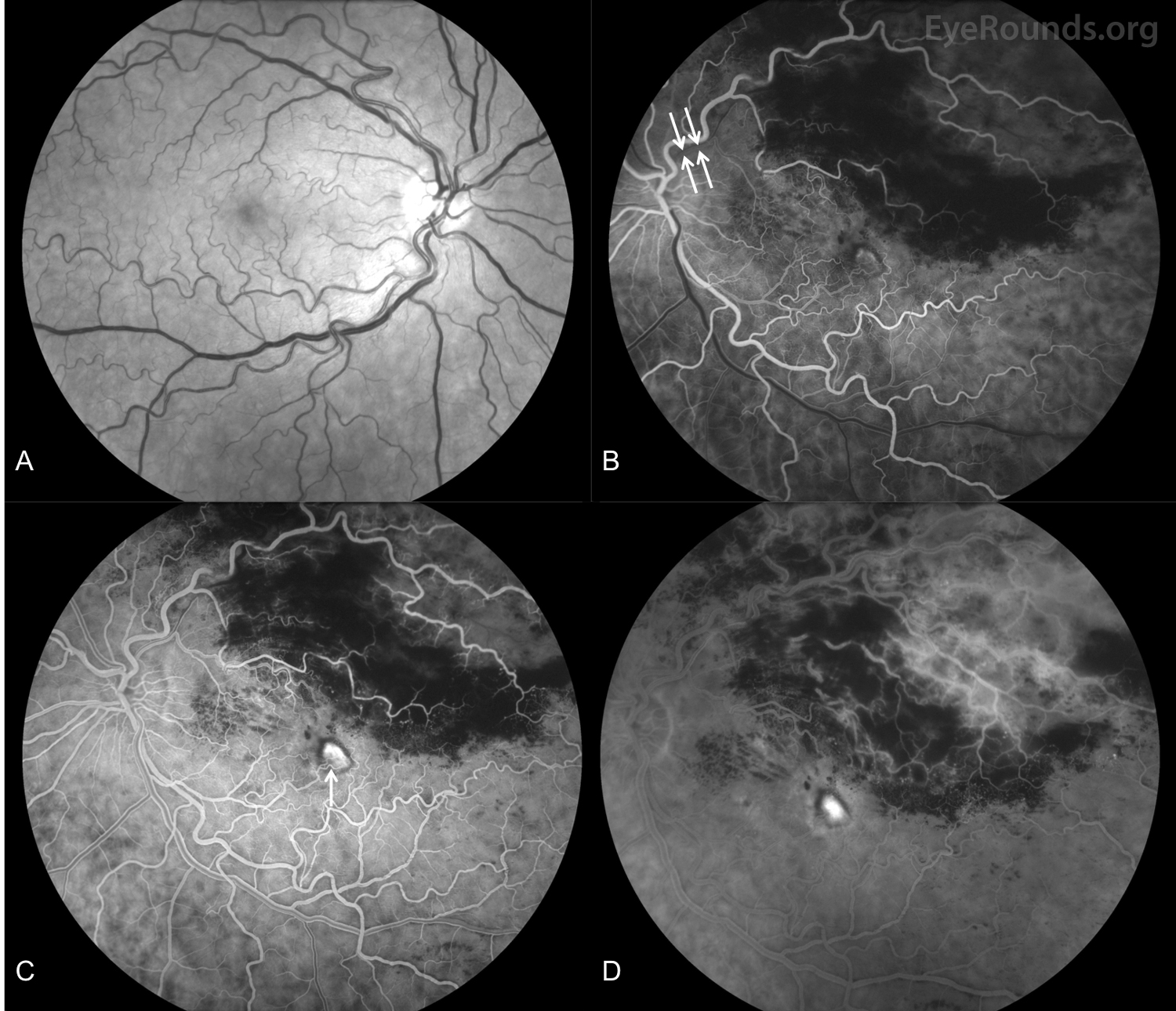
Figure 2. Fundus fluorescein angiography (FFA), both eyes: A. There was no evidence of vasculitis or leakage in the right eye. B-D. In the left eye, there was attenuation of the superotemporal veins (B), early staining of the central lesion (C, arrow) with late leakage (D), prominent superotemporal leakage (D), and no leakage inferotemporally. There was blockage superotemporally corresponding to the intraretinal hemorrhages. There was decreased perfusion and capillary remodeling of the far superotemporal peripheral vasculature (C and D).
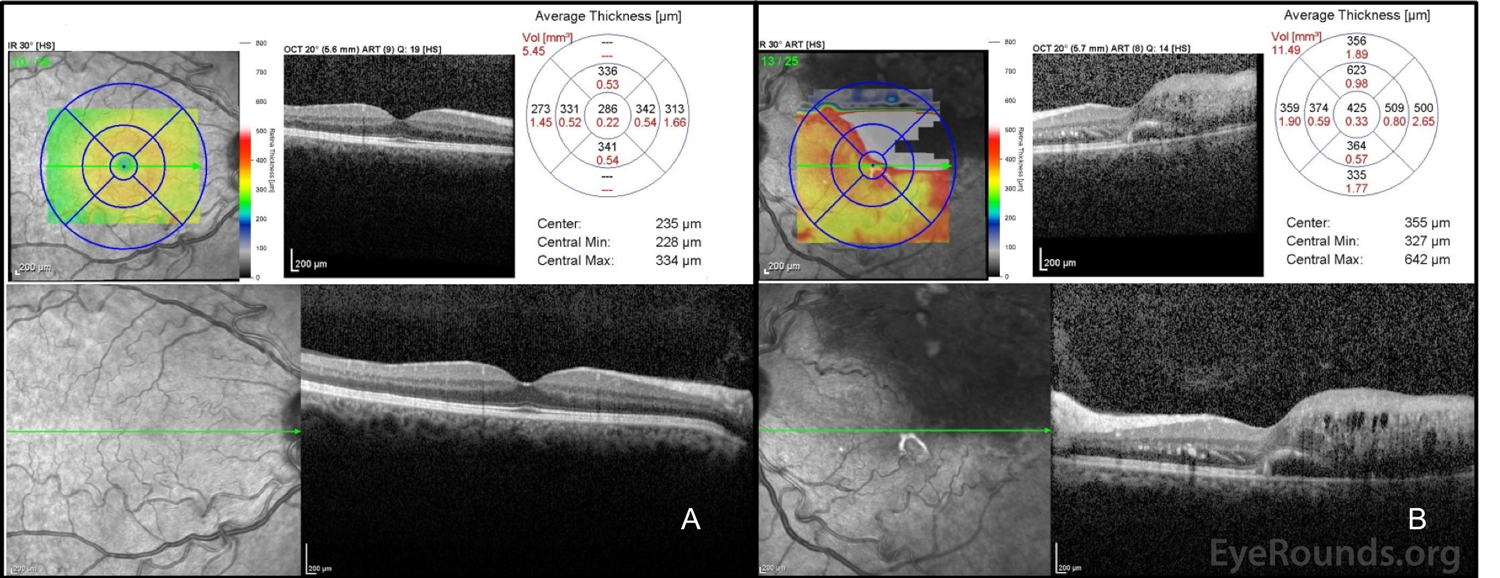
Figure 3. Optical coherence tomography (OCT): A. In the right eye, the central macular thickness (CMT) was 286 microns with a normal foveal contour. B. In the left eye (OS), the CMT was 425 microns with marked cystoid macular edema superiorly with subretinal fluid superiorly and temporally. Not depicted here is a pigment epithelial detachment inferior to the fovea with isodense material OS.
Funduscopic exam in the comprehensive ophthalmology clinic was significant for a recurrent superotemporal BRVO. Fundus photography (Figure 1), fundus fluorescein angiography (FFA; Figure 2), and optical coherence tomography (OCT; Figure 3) were promptly obtained, and the patient was evaluated by the retina service on the same day. An anti-VEGF intravitreal injection was recommended at that time given the presence of massive macular edema OS; however, the patient was unable to stay for the injection and arrangements were made for patient to follow-up in one week. Follow-up with the patient's primary care physician was recommended for blood pressure monitoring and control.
At the one-week follow-up, the patient reported no new symptoms and reported that her vision remained unchanged. OCT showed increased central macular thickness (CMT) from 425 microns to 550 microns. There was also an increase in subretinal fluid (SRF) and intraretinal fluid (IRF) involving the fovea in addition to subfoveal, hyperreflective material. The patient received a 0.5 mg ranibizumab (Lucentis®) intravitreal injection. She was scheduled for a follow-up appointment and a repeat ranibizumab injection in 4-5 weeks.
Despite a lack of hypertension on clinic testing, hypertensive retinopathy was also present given the striking AV nicking and vessel tortuosity in both eyes (Figure 1). Due to the history of stroke in her early 50s, relatively early onset for first BRVO (54 years of age), and recurrence of BRVO, further work-up with laboratory studies were performed to elucidate an underlying cause. The work-up included 24-hour ambulatory BP monitoring, a formal sleep study, and labs to assess for diabetes, clotting disorders, and other possible conditions (see below for complete work-up). Based on this work-up, it was determined that the patient had Factor V Leiden thrombophilia due to a missense mutation. She was then referred to the hematology service and was continued on aspirin therapy.
The patient was followed closely every 1-2 months for intravitreal injections in the left eye. Her visual acuity improved to 20/25 OS within six months of initiating this injection schedule. However, the patient lost her insurance and was subsequently lost to follow-up for approximately five months. Upon return, the patient's visual acuity in the left eye had decreased to 20/200, and she was noted to have retinal neovascularization (NV) and recurrence of massive CME in the left eye (Figures 4 and 5). The patient underwent panretinal photocoagulation (PRP) and an intravitreal injection of Avastin OS.
-Cholesterol: 266 mg/dL
-HDL: 128 mg/dL
-TG: 120 mg/dL
-LDL: 104 mg/dL
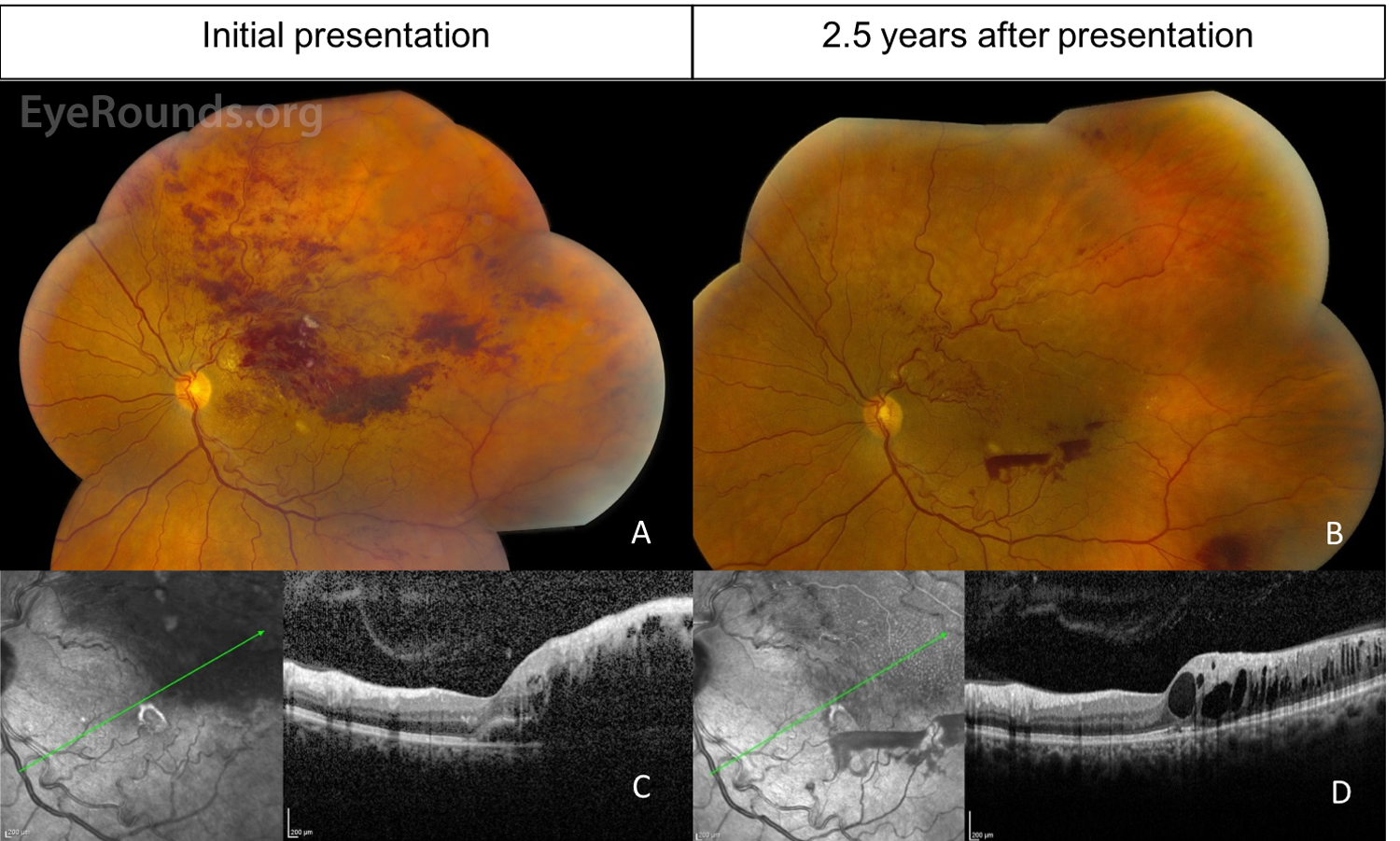
Figure 4. Color fundus photography, left eye: A. At her initial presentation to UIHC, there was a recurrent superotemporal BRVO along the superior arcade with massive intraretinal and retinal nerve fiber layer hemorrhages. B. At her most recent visit 2.5 years later, there were scattered intraretinal hemorrhages in the macula in addition to regions of NV in the superior macula and preretinal hemorrhages temporally and inferotemporally. Superotemporal sclerotic vessels were present. There was an area suspicious for an inferotemporal retinal arterial macroaneurysm in the mid-periphery. C-D. OCT showed improvement of subretinal fluid, but there was still persistence of intraretinal fluid when comparing the initial (C) and most recent (D) OCT images. The persistent of fluid with new NV was likely a result of the patient missing several appointments.
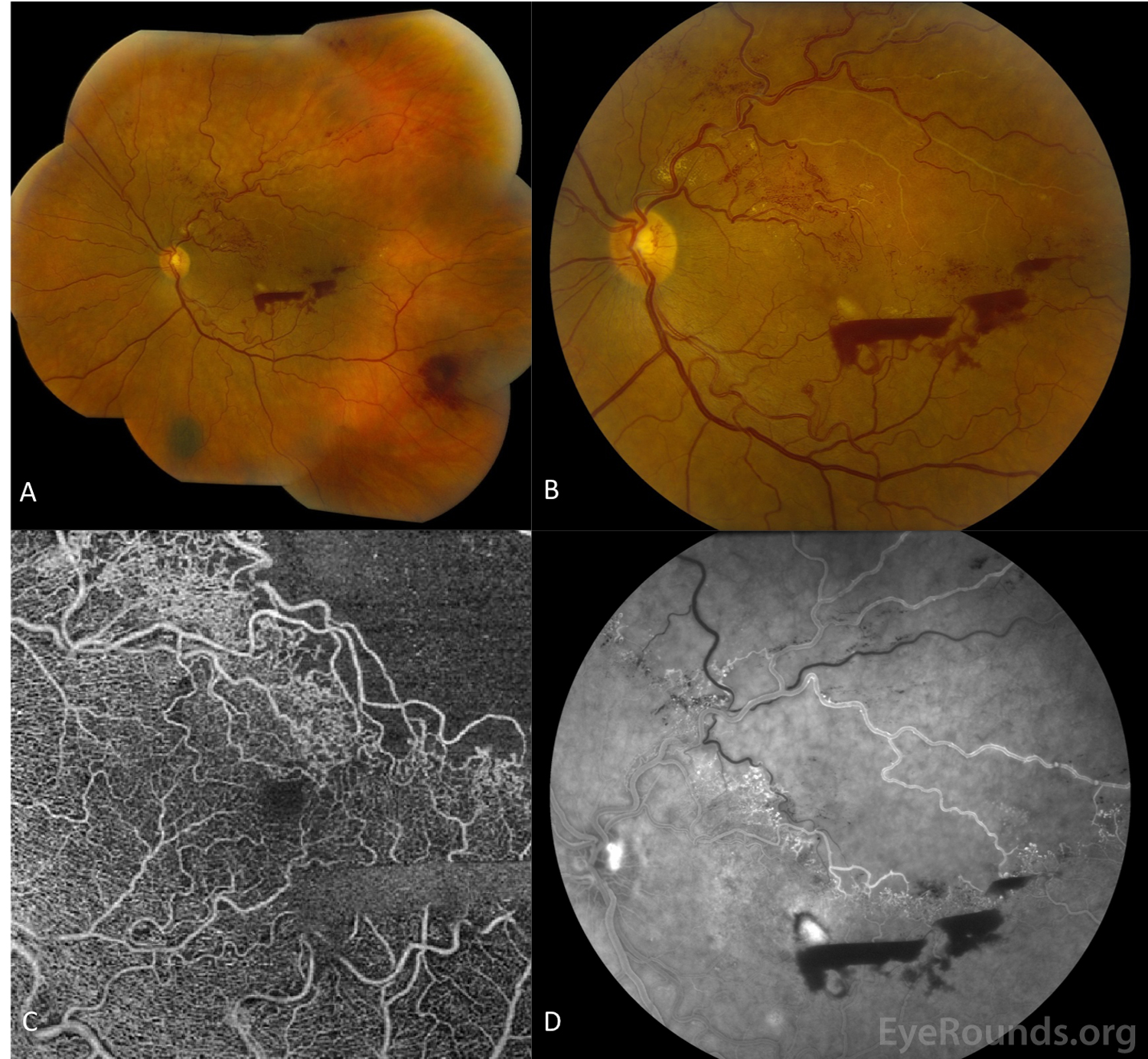
Figure 5. Retinal neovascularization on follow-up examination, OS: The patient had a significant decrease in vision from 20/25 to 20/200 after she missed several appointments. On fundus exam, there was a recurrence of hemorrhages (A) and persistence of fluid with new regions of NV in the superior macula (B). OCT angiography (OCT-A) was obtained (C), and this image modality showed capillary and large vessel dropout in the superotemporal macula in the region of the prior BRVO. Retinal NV in the inner retina was evident using OCT-A. Fundus fluorescein angiography (D) showed superotemporal non-perfusion with evidence of leakage from NV and collateral vessels in the superior macula in addition to the disc with blockage of stain by the central, preretinal hemorrhages.
A retinal vein occlusion (RVO) is one of the most common types of retinal vascular disease, second only to diabetic retinopathy [1]. RVOs are classified based on location of the obstruction. For example, a branch RVO (BRVO) affects one of the branches of the central retinal vein, whereas a hemispheric RVO (HRVO) affects a trunk of the central retinal vein draining the superior or inferior retinal hemisphere. A central RVO (CRVO) occludes the central retinal vein proper. BRVO can be further classified as major or macular depending on the anatomical location. Major BRVO refers to an occlusion of a retinal vein that drains one of the quadrants, and macular BRVO refers to an occlusion of a venule within the macula. Venous obstruction may be sufficiently severe to cause non-perfusion and macular ischemia. RVOs can be further characterized as non-ischemic (i.e., perfused) or ischemic (i.e., non-perfused) depending on the status of retinal perfusion. BRVO is generally considered to be ischemic whenever there is an area of retinal capillary non-perfusion of five disc areas or greater on fluorescein angiography [2]. Perfusion status has important implications in therapy and prognosis, as discussed below [2].
Although the exact mechanism of BRVO has not been completely elucidated, BRVO is thought to follow the principle of Virchow's triad for intravascular thrombus formation, such that there is endothelial damage, hemodynamic changes in blood flow, and hypercoagulability. The majority of patients with BRVOs have underlying systemic arterial disease [3]. Chronic conditions such as hypertension, diabetes mellitus, and hyperlipidemia result in arteriosclerosis, a process that is characterized by thickening and hardening of the arterial wall with a loss of elasticity. BRVO predominantly occurs at AV crossings (Figure 1, arrowheads), where thick-walled arteries compress and obstruct adjacent thin-walled veins, a process that is likely exacerbated by underlying retinal arterial disease. Given that a greater number of AV crossings are present in the superotemporal region, approximately two thirds of major BRVO occur in the superotemporal quadrant, followed by the inferotemporal quadrant and less commonly in the nasal quadrants [3-6]. Retinal arterioles are found anterior to venules nearest the occlusion in the majority of eyes with BRVO [4]. Several studies have shown that compression by the artery causes trophic changes to the venous endothelium with evidence of tunica intima and medial layer hypertrophy [7]. Turbulent hemodynamic changes also occur due to the abrupt change in blood flow direction and contribute to thrombogenesis [3, 4]. Prothrombotic conditions, including hyperviscosity syndromes, vasculitides, and hypercoagulable states, such as in our patient, have also been implicated in BRVO [3, 8, 9].
Complications of BRVO include cystoid macular edema (CME), macular ischemia, retinal neovascularization (NV), vitreous hemorrhage, and retinal detachment. BRVO-associated CME is likely multifactorial. Increase in hydrostatic pressure in the obstructed and congested vein results in escape of intravascular fluid across the vessel wall. Reduced venous flow results in reduced capillary perfusion and ischemia, leading to upregulation of hypoxia-inducible factor 1α (HIF-1α). HIF-1α upregulates expression of endothelin-1 and vascular endothelial growth factor (VEGF), which promotes endothelial permeability. Such permeability contributes to the breakdown of the blood-retina barrier and leads to CME. Thus, increased levels of VEGF are associated with a greater degree of CME and ischemia. Inflammation is thought to contribute to increased endothelial permeability and edema as well. Elevated levels of pro-inflammatory cytokines, including IL-6 and IL-8, have been detected in the vitreous in eyes affected by BRVO [3]. Although the goal of VEGF is to promote perfusion to ischemic areas through angiogenesis and NV, the newly-formed vessels possess immature, "leaky" walls, contributing to CME and increasing the risk of vitreous hemorrhage (3). Levels of VEGF correlate with the size of the area of retinal non-perfusion, and the risk of NV increases proportionally to the size of the area of non-perfusion [2, 3]. Approximately 20% of BRVO cases go on to develop retinal NV [10].
BRVO is the most common type of RVO with an incidence of 0.5% to 1.2% [3]. Men and women are affected equally [3, 5, 11]. There is a slightly higher incidence in patients of Asian ethnicity, as well as in the Hispanic population [3]. In a meta-analysis combining data from 11 studies across the world and involving 49,869 subjects, the RVO prevalence was 5.20 per 1000, of which BRVO accounted for 4.42 cases per 1000 [11]. In the United States, 180,000 eyes are affected by RVO annually, and up to 80% are due to BRVO [11, 12]. The prevalence of BRVO increases with age: 4.58 cases per 1000 in the fifth decade, 11.11 per 1000 in the sixth decade, and 12.76 per 1000 in seventh decades of life [11].
In addition to advancing age, BRVO risk factors include conditions causing systemic arterial disease such as hypertension, hyperlipidemia, diabetes mellitus, and smoking. The prevalence of hypertension in BRVO has been reported to be around 48% and is significantly higher compared to the prevalence of hypertension in CRVO [7]. The prevalence of diabetes mellitus in CRVO is significantly higher compared to the prevalence of diabetes mellitus in BRVO; however, BRVO patients have an increased prevalence of diabetes compared to that of non-RVO controls [7, 13]. Hyperviscosity syndromes, vasculitides, and other hypercoagulable states also increase the risk of BRVO [3, 10]. Nasal BRVOs are far less commonly noticed than temporal BRVOs, but they have been shown to share the same epidemiological characteristics [14].
BRVO typically presents as either an acute and painless decrease in visual acuity, partial visual field defect, or monocular visual distortions with blurred or gray vision corresponding to the location of BRVO. Occlusions not involving the macula may be asymptomatic and diagnosed on routine ophthalmologic examination. Some patients may present with "floaters" due to a vitreous hemorrhage. In contrast, patients with a CRVO are seldom asymptomatic. Occlusions affecting the macula may result in significant morbidity, with visual acuity decreased to count fingers [3].
Research shows that visual acuity is usually only affected in temporal BRVO with nasal BRVO typically being asymptomatic. Hayreh, et al. reported that initial temporal BRVO visual acuity was 20/70 or worse in 49% of eyes [6]. Visual field defects in temporal BRVO are minimal to mild in 72% and moderate in 26% of eyes. There is no difference between superotemporal and inferotemporal BRVO visual acuities or visual field defects [6]. Patients with chronic BRVO may present with typical signs and symptoms of neovascular glaucoma (NVG) as a complication of chronic retinal hypoxia [15].
BRVO diagnosis is made clinically and can be further characterized by imaging. Fundus examination reveals dot-blot and flame hemorrhages in the characteristic distribution of the occluded vein (Figure 1). A hemorrhage at the affected AV crossing, termed the Bonnet sign, may be seen. The occluded vein may be widened and congested distal to the obstruction at the AV crossing with hemorrhages in the draining territory; the vein may be narrowed and flat proximal to the obstruction. Cotton wool spots may be present, and CME may be appreciated on exam [10].
Imaging tests, including fundus fluorescein angiography (FFA) and optical coherence tomography (OCT), aid in the diagnosis, assessment of severity, and follow-up plans. FFA characteristically reveals delayed filling of the occluded vein (Figure 2); this image modality confirms the clinical diagnosis and is helpful in assessing for presence and degree of macular edema and macular non-perfusion. Initially, perfusion status may be difficult to ascertain due to blocking secondary to a large hemorrhage. In such cases, FFA may need to be repeated following adequate hemorrhage clearing [10]. NV may be seen in more chronic cases, characterized by fluorescein leak and by presence of collateral vessels crossing the horizontal raphe.
OCT permits detection of CME and accurate, objective measurement of CMT (Figures 3 and 4). Unlike FFA, it is not impeded by the presence of hemorrhage. It is particularly helpful in monitoring disease progression and response to therapy. Optical coherence tomography-angiography (OCT-A) can be used to provide detailed images or retinal vasculature and pathologic structures to analyze patterns to help distinguish perfused from non-perfused areas in BRVO [16-19]. OCT-A may also be used to further characterize choroidal NV that occurs as a complication of disorders that cause retinal hypoxia (Figure 5C).
Goldmann perimetry is not routinely performed in patients with BRVO but may reveal arcuate scotomas, central scotomas, paracentral scotomas, and segmental peripheral constriction. However, many patients with chronic BRVO may present with secondary NVG for which visual fields should be routinely evaluated. BRVO-related scotomas may complicate the interpretation of glaucomatous-related visual field defects. In a recent study by Hayreh, et. al, the Amsler grid detected areas of metamorphopsia in 20 BRVO eyes that had no identifiable central lesion on kinetic perimetry [6]. A relative afferent pupillary defect (RAPD) may occur in the setting of severe BRVO and BRVO-related NVG due to severe retinal ischemia and optic nerve damage, respectively [20].BRVO treatment focuses on reducing CME, preventing NV, and treating NV to reduce risk of vitreous hemorrhage. The current gold standard treatment is laser photocoagulation based on the landmark Branch Vein Occlusion Study (BVOS). In this multicenter, prospective, randomized, controlled clinical trial published as two reports in 1984 and 1986, investigators assessed whether peripheral scatter argon laser photocoagulation could prevent the development of NV and vitreous hemorrhage by applying treatment over the entire involved segment and extending no closer than two disc diameters from the foveal center. Authors also sought to determine whether grid-pattern laser photocoagulation was useful in improving visual acuity in the eyes with BRVO-associated CME; treatment was applied over the area of macular capillary leakage no closer to the fovea than the avascular zone and not extending beyond the vascular arcades [1, 2].
In the eyes with ischemic BRVO, defined as greater than five disc diameters of non-perfusion, and no NV at baseline, patients treated with sector laser photocoagulation developed NV less frequently than the patients in the control group (Table 1). In eyes with retinal NV at baseline, sector laser photocoagulation reduced occurrence of vitreous hemorrhage (Table 1). Grid-pattern laser photocoagulation significantly improved vision in eyes with visual acuity less than 20/40 due to macular edema in non-ischemic BRVO (Table 2). The BVOS Study Group recommended grid-pattern laser treatment in cases where CME explained visual loss with visual acuity of 20/40 or worse, a follow-up at four-month intervals in cases of retinal non-perfusion of five disc diameters or greater to look for development of NV, and sector laser treatment in cases where NV had developed [1, 2].
|
Ischemic BRVO initially without NV that later developed NV |
Ischemic BRVO with NV that later developed vitreous hemorrhage |
Sector laser group |
12% |
29% |
Control group |
22% |
61% |
Table 1: BVOS outcomes for ischemic BRVO with and without baseline neovascularization treated with sector laser photocoagulation [1, 2].
Abbreviations: BVOS, branch vein occlusion study; BRVO, branch retinal vein occlusion; NV, neovascularization
|
Non-ischemic BRVO with macular edema and VA less than 20/40 that gained > 2 lines |
Grid-pattern laser group |
65% |
Control group |
37% |
Table 2: BVOS outcomes for non-ischemic BRVO with macular edema treated with grid-pattern laser photocoagulation [1, 2].
Abbreviations: BVOS, branch vein occlusion study; VA, visual acuity
Recognition of VEGF as an important player in BRVO pathophysiology prompted investigation into anti-angiogenic agents already in use for treatment of neovascular age-related macular degeneration. The 2010 Branch Retinal Vein Occlusion (BRAVO) study examined the outcomes of intravitreal anti-VEGF injections for treatment of BRVO [12]. In this randomized, sham injection-controlled clinical trial, patients with BRVO-associated CME received intraocular injections of 0.3 mg or 0.5 mg ranibizumab (Lucentis®). The improvement in visual acuity was dramatic following the first injection of ranibizumab using either dose. Furthermore, treatment with ranibizumab for six months effectively treated macular edema, ranibizumab-treated patients having less CME compared to the patients in the sham group (Table 3) [12]. The more recent phase III VIBRANT trial demonstrated that aflibercept (Eylea®) is safe and effective for CME secondary to BRVO in comparison to grid laser [21]. Bevacizumab (Avastin®) is also commonly used for this purpose, and there are multiple small retrospective studies and prospective trials, such as the multicenter, randomized, controlled SCORE2 trial, showing the efficacy of this intravitreal drug [22, 23]. Both ranibizumab and aflibercept are FDA approved for BRVO-related CME, whereas the use of bevacizumab in 2018 is considered to be an off label medication for this indication.
|
Mean improvement in VA at 7 days |
Mean improvement in VA at 6 months |
Percent of eyes with VA improved of 3 or more lines at 6 months |
Percent of eyes with macular edema resolution at 6 months |
Ranibizumab 0.5 mg group |
7.5 lines |
3-4 lines |
61% |
91% |
Ranibizumab 0.3 mg group |
7.5 lines |
3-4 lines |
55% |
85% |
Sham injection control group |
0 lines |
1.5 lines |
29% |
45.5% |
Table 3: The BRAVO study outcomes for BRVO treated with ranibizumab vs. sham injection [12].
Abbreviations: BRAVO, branch retinal vein occlusion; BRVO, branch retinal vein occlusion; VA, visual acuity
The use of intravitreal corticosteroid injection as an alternate treatment for BRVO is based on the results of the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) Trial, which was published as a series of reports [24]. The rationale for this prospective, randomized clinical trial was based on the evidence that corticosteroids inhibit VEGF expression and decrease the inflammatory response implicated in macular edema development. The 2009 SCORE 6 study compared 1 mg and 4 mg triamcinolone acetate intravitreal injections to grid-pattern laser photocoagulation in treating BRVO. There was no significant difference between the treatments when comparing visual acuity improvement from baseline (Table 4). Intravitreal corticosteroids featured a worse side effect profile, including cataract development and/or progression and increased intraocular pressure [24]. Nevertheless, intravitreal corticosteroids, including triamcinolone, fluocinolone, and dexamethasone, constitute an additional treatment option in BRVO therapy and have utility in a subset of BRVO patients, such as pseudophakic patients or patients in whom anti-VEGF treatments are inadvisable, such as pregnant patients. A slow-release biodegradable intra-ocular implant releasing dexamethasone (Ozurdex®) has been tested in the Global Evaluation of implaNtable dExamethasone in retinal Vein occlusion with macular edemA (GENEVA) Trial [25]; given the strong evidence for its safety and efficacy in this multicenter, sham-controlled clinical trial, Ozurdex is now an FDA-approved treatment of CME in the setting of RVO [26].
|
Percent of eyes with VA improvement of at least 15 letters at 12 months |
Triamcinolone acetate |
27.2% |
Triamcinolone acetate |
25.6% |
Grid-pattern laser photocoagulation |
28.9% |
Table 4: The SCORE 6 study outcomes for BRVO treated with corticosteroid injection (24).
Abbreviations: SCORE, standard care vs corticosteroid for retinal vein occlusion; VA, visual acuity
Based on the above evidence, current BRVO treatment follows a series of decisions. Initially, a determination is made as to the cause of decreased visual acuity. If visual loss is due to macular edema, early treatment with intravitreal anti-VEGF injections is recommended given strong evidence for the safety and efficacy of these injections [22]. Grid-pattern macular photocoagulation is no longer routinely performed for CME from BRVO given the ease and success of anti-VEGF injections in this setting. Additionally, there is a lag in visual acuity improvement with grid laser compared to anti-VEGF injections [22]. Steroid injections or a steroid implant are alternatives to anti-VEGF in the event that a patient is pseudophakic, is not a steroid responder, has failed anti-VEGF therapy, and/or has a need for longer acting therapy. In patients with a significant area of non-perfusion (i.e., five disc diameters or greater), a regular follow-up is recommended at least every four months for detection of NV development. If NV is present, laser photocoagulation of the involved sector is recommended [2, 10]. For details regarding additional treatment options, including vitrectomy and systemic hemodilution, a comprehensive review of BRVO treatment options was recently published by Ehlers, et al. as an American Academy of Ophthalmology report [22]. Table 5 provides an outline of selected BRVO clinical trials for reference.
Clinical Trial |
Study Design |
Treatment Groups |
Conclusions |
Ref |
Branch Vein Occlusion Study (BVOS)a |
Multicenter, prospective RCT |
Sector laser photocoagulation vs. No laser for non-ischemic or ischemic BRVO for prevention of NV development |
|
[1 ,2] |
Branch Retinal Vein Occlusion Study (BRAVO)b |
Multicenter, double-masked, prospective, Phase III RCT |
Ranibizumab (Lucentis®) intravitreal injections (0.3 mg or 0.5 mg) vs. Sham injections for BRVO-associated CME |
|
[12] |
VIBRANT trial |
Double-masked, Phase III RCT |
Aflibercept (Eylea®) intravitreal injection vs. Grid-pattern laser for BRVO-associated CME with Aflibercept/laser combination group in second half of study |
|
[21] |
Study Evaluating Dosing Regimens for Treatment with Intravitreal Ranibizumab Injections in Subjects for CME following RVO (SHORE) Trial |
Masked, prospective RCT |
Ranibizumab (Lucentis®) as needed or monthly intravitreal injections for BRVO or CRVO-associated CME |
|
[27] |
MAcular edema due to branch Retinal Vein OccLusion (MARVEL) Trial |
Double-masked, prospective, non-inferiority RCT |
Ranibizumab (Lucentis®) vs. Bevacizumab (Avastin®) intravitreal injections in BRVO-associated CME |
|
[28] |
SCORE2 Trial |
Multicenter, non-inferiority prospective RCT |
Bevacizumab (Avastin®) vs. Aflibercept (Eylea®) in CRVO or HRVO-associated CME |
|
[23] |
Standard Care vs. Corticosteroid for Retinal Vein Occlusion (SCORE) Trialc |
Multicenter, prospective RCT |
Triamcinolone acetate intravitreal injections (1mg or 4mg) vs. Grid-pattern laser for BRVO |
|
[24] |
Global Evaluation of implaNtable dExamethasone in retinal Vein occlusion with macular edemA (GENEVA) Trial |
Multicenter, masked, prospective RCT |
Dexamethasone (0.35mg or 0.7mg) intra-ocular implant vs. Sham injection for CME in RVO |
|
[25] |
Table 5. Overview of Selected BRVO clinical trials.
aTwo study reports were published in 1984 and 1986. In the earlier report, the authors sought to determine whether grid-pattern laser photocoagulation was useful in improving visual acuity in the eyes with BRVO-associated CME. The later report focused on whether laser photocoagulation could prevent the development of NV and vitreous hemorrhage.
bThe HORIZON trial was the 12-month open-label extension of the BRAVO trial. The RETAIN trial was the 49-month open-label extension of the BRAVO trial.
cThe SCORE Trial was published as a series of reports. The SCORE Trial information in this table refers to the 2009 SCORE 6 study.
Abbreviations: BRVO, branch retinal vein occlusion; CME, cystoid macular edema; CRVO, central retinal vein occlusion; HRVO, hemiretinal vein occlusion; NV, neovascularization; PRN, pro re nata; RCT, randomized, controlled clinical trial; RVO, retinal vein occlusion; VA, visual acuity; VH, vitreous hemorrhage
BRVO consists of two distinct entities, including major BRVO and macular BRVO, which typically each demonstrate a favorable prognosis [6, 29]. Hayreh, et al. studied the natural history of 216 untreated eyes, andthey reported that major BRVO with an initial VA of 20/70 or worse and a median initial VA of 20/200 improved to 20/50 at 15 months follow-up in untreated eyes [6]. In eyes with macular BRVO, the VA does not improve as much as in the major BRVO [6].
The author also reported an overall improvement from initial VA for major BRVO and macular BRVO, which is presented in Table 6 [6, 29]. Visual field defects that occur in temporal BRVO and macular BRVO improve in the majority of patients [6, 29]. The median time to CME resolution in major BRVO and macular BRVO was 21 months and 18 months, respectively [6, 29]. However, the median time for complete BRVO resolution (i.e., no CME and no retinal hemorrhages) was 4 and 1.5 years, respectively [6]. In general, younger age has been shown to be significantly associated with improved VA outcomes [6, 29]. A lack of improvement in some eyes may be attributable to permanent ischemic damage to macular retinal ganglion cells and pigmentary changes in the foveal region due to prolonged macular edema [6, 29].
Initial VA of 20/70 or worse |
Initial VA of 20/60 or better |
|
Percent of major BRVO with stable or improved VA |
69% |
75% |
Percent of macular BRVO with stable or improved VA |
53% |
87% |
Table 6: Percent of major and macular BRVO patients with stable or improved VA at 15 months follow-up according to initial VA [6, 29]. Abbreviations: BRVO, branch retinal vein occlusion; VA, visual acuity
Ocular NV occurs in the setting of retinal ischemia and typically involves the retina, iris, and anterior chamber angle resulting in NVG. This subtype of glaucoma has a poor prognosis and may result in ocular morbidity, including unremitting elevated intraocular pressure with profound visual loss that is often unresponsive to medication and/or surgery [20]. Other complications include vitreous hemorrhage and tractional retinal detachment.
It remains unclear if RVO is associated with cardiovascular disease. A recent retrospective 12-year nationwide cohort study from the Korea National Health Insurance Service found that central or branch RVO is associated with an increased risk of ischemic, but not non-ischemic, heart failure [30]. Another retrospective cohort study found no increased risk for ischemic heart disease; however, the event rate of cerebral vascular accidents was almost 2-fold in patients with RVO compared to controls [31]. In another large population-based study, RVO was not associated with cardiovascular or cerebrovascular-related mortality [32]. A recent population-based retrospective cohort study using the entire population of the Taiwan National Health Insurance Research Database (37921 subjects with RVO) calculated the hazard ratio (HR) for developing acute myocardial infarction (AMI); although there was a significantly higher adjusted HR in the BRVO group (HR 1.15; p=0.0005) compared to controls (HR 1.0), the CRVO group (HR 1.35) had a significantly higher risk of AMI than the BRVO group (p<0.01) and the control group (p<0.0001) [13].
Up to 10% of patients with BRVO in one eye will develop any type of RVO in the fellow eye [2]. Thus, preventive measures play an important role in the care of a patient with BRVO and include controlling modifiable risk factors, such as hypertension, hyperlipidemia, body mass index, and diabetes mellitus. Given that some studies suggest a higher prevalence between newly diagnosed BRVO and ischemic heart disease, the presence of the aforementioned risk factors may merit a cardiology consultation.
In cases where BRVO occurs in a young patient, a patient with no identifiable arterial disease risk factors, or a patient with recurrent occlusions, a further work-up is warranted to seek for other causes of BRVO. The diagnosis and treatment of other etiologies is typically pursued in collaboration with the patient's primary care physician as well as a hematologist, and treatment is aimed at preventing further retinal vascular events [10]. A rare and poorly understood entity called Susac's syndrome is a subtype of primary angiitis of the central nervous system (PACNS) and is associated with the clinical triad of visual loss caused by BRVO, sensorineural hearing loss, and subacute encephalopathy. This disease presents with hyperintense lesions in the corpus callosum on T2-weighted magnetic resonance images and requires early treatment with immunosuppressive agents to prevent irreversible vision loss in the future [33].
Our patient's case is complicated by a prior history of AMD OS with an associated choroidal neovascular membrane, one prior episode of BRVO OS, and a history of stroke with a reported visual field defect OS that subsequently improved. Although the patient denied a history of hypertension and was normotensive in our clinic, her fundoscopic exam featured striking vessel tortuosity and AV nicking typically seen in the setting of long-standing hypertension. This, along with a prior history of stroke, a factor V Leiden mutation, and a prior history of smoking suggests both arterial vascular disease and hypercoagulability as the most likely causes of the current BRVO. There are several case reports and case series that suggest a factor V Leiden mutation, like other pro-thrombotic states, increases the risk for recurrent BRVOs [8, 9]. Our patient had previously quit smoking, a commendable modification of a risk factor. The patient was also counseled on the importance of regular blood pressure monitoring and control, as needed, in collaboration with her primary care physician. She has also started taking a daily aspirin, and she has been referred to a hematologist. She will continue follow-up with the retina specialists for further treatment of the current BRVO.
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Scruggs BA, Quist TS, Kravchuk O, Sohn EH. Branch Retinal Vein Occlusion. EyeRounds.org. posted July 20, 2018; Available from https://EyeRounds.org/cases/274-branch-retinal-vein-occlusion.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
