Chief Complaint: Diplopia, pain with eye movement, nausea and vomiting
History of Present Illness: The patient was a 17-year-old male who was involved in a physical altercation that resulted in a closed fist blow to the left side of his face. He immediately noted double vision with both eyes open. Subsequently, he experienced significant pain when attempting to look up and had associated nausea and vomiting.
Best Corrected Visual Acuity (BCVA): Right eye (OD): 20/20, Left eye (OS): 20/20
Intraocular pressure (IOP): OD: 20 mmHg, OS: 19 mmHg
Pupils: no RAPD, both eyes (OU)
Visual Fields: Full to confrontation, OU
Hertel Exophthalmometry: Base 104 mm; right eye (OD): 19 mm, left eye (OS) 16 mm
External Exam: minimal periorbital edema, no ecchymosis
Slit lamp exam (OS): few scattered, small sub-conjunctival hemorrhages OS, otherwise normal OU
Ocular motility: Left hypotropia in primary gaze. OD: full motility, OS: Significantly reduced supraduction and pain when looking up (see figure 1). Patient became nauseated during the ocular motility testing. Restriction on forced supraduction OS compared with OD
Dilated fundus exam: normal OU
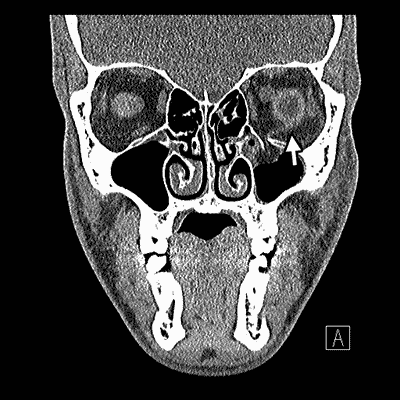
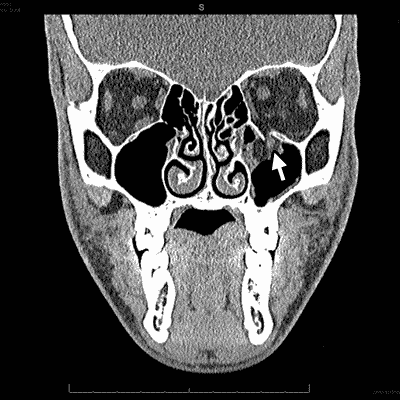
Maxillofacial computed tomography (CT): (see figure 2)
|
Based on history, clinical exam and CT imaging, the patient was diagnosed with a left orbital floor fracture with entrapment. He was taken to the operating room for surgical repair within 8 hours of presentation. Forced ductions showed marked limitation to elevation of the left eye. A transconjunctival approach was used to expose the inferior orbital wall fracture and entrapment of the inferior rectus was confirmed. The entrapped orbital tissues were released. Subsequent forced ductions were normal. A 0.4mm Supramid implant was used to cover the floor defect and secured with titanium screws along the inferior orbital rim. At the one week follow-up visit, the patient was noted to have 6 prism diopters of left hypertropia, mild diplopia in all gaze directions and mild deficits in up and down gaze of the left eye (see figure 3). At the one month follow-up visit, the patient was noted to have 20/15 visual acuity, no diplopia, full extraocular movements and no enophthalmos.
Orbital blowout fractures are caused by hydraulic mechanisms transmitting force through orbital soft tissue into the orbital walls, direct buckling mechanisms as the result of deformation of the bony orbital rim, or a combination of the two (1). In adults and children, the medial and inferior orbital walls are the most vulnerable to fracture (2-4) due to their thin bone structure.
Signs and symptoms of orbital floor fractures include orbital pain, enophthalmos, hypesthesia in the V2 distribution (due to damage to the infraorbital nerve) and vertical diplopia. Associated signs may include eyelid ecchymosis, subcutaneous emphysema, ptosis, pupillary dilation, and epistaxis (5).
Exam and workup should be modified to detect the common sequelae mentioned above. Visual acuity and pupils should be checked. If there is a relative afferent pupillary defect, this may indicate a traumatic optic neuropathy. Intraocular pressure can raise or lower suspicion for a retrobulbar hemorrhage causing an orbital compartment syndrome. Hertel exophthalmometry is used to quantify the presence of exophthalmos or enophthalmos. It is extremely important to ask about diplopia and perform careful assessment of extraocular motility and forced ductions (if necessary) to detect orbital tissue entrapment or extraocular muscle paralysis. Slit-lamp examination is used to diagnose co-morbidities of ocular trauma including corneal abrasion, hyphema, traumatic iritis, iridodialysis, iris sphincter tears, lens dislocation, cataract, vitreous hemorrhage, or a ruptured globe. Finally, fundus examination is used to diagnose retinal tears, detachment or commotio retinae (5).
For many orbital floor fractures, a 1-2 week window of observation has been suggested prior to repeat exam (6). This allows time for clearing of edema and hemorrhage, which can mask latent enophthalmos and motility deficits. This observation period enables the ophthalmologist to determine which patients will benefit most from surgical intervention. Surgical intervention for orbital floor fractures consists of releasing the herniated orbital tissue (fat, muscle or both) that may be found in the fracture site back to its normal orbital position in order to improve motility. This is followed by repair of the floor defect in order to improve normal orbital volume and anatomic relationship (1). A fibrotic response to the initial injury can continue to progress over several months. In turn, prolonged observation can make late repair more difficult and less successful.
The need for immediate surgery (within hours) after orbital floor fracture occasionally arises. One such scenario is when the globe herniates into the maxillary sinus. Another clinical scenario that may benefit from urgent surgery within hours to days is the whited-eyed blowout fracture (WEBOF), formally described by Jordan et al. The WEBOF is seen in young patients with little or no clinical evidence of soft tissue trauma (edema, ecchymosis). There is diplopia with restriction of vertical gaze, lack of enophthalmos and radiologic signs of minimal, if any, bone displacement. There may or may not be signs of orbital tissue herniation into the maxillary sinus on imaging (1).
When adults sustain an orbital floor fracture, the floor more commonly buckles and breaks in several areas and a portion of the floor "blows out" and displaces with residual open communication into the maxillary sinus. Because children have less bony calcification, they have softer, more flexible bones and the orbitval floor is more likely to bend, crack and form a flexible trap door, which can lead to entrapment of orbital tissue (1).
Because there are often few external and radiologic signs, the WEBOF can be easily overlooked (7). Diagnosis may be delayed further by patient’s symptoms of nausea and vomiting which can lead to radiologic investigation of the head, rather than the orbit, in search of intracranial injury. Lane et al found that WEBOF patients were less likely to undergo orbital imaging in the emergency room, more likely to be diagnosed with concussion, less likely to be seen urgently by an ophthalmologist and were told to follow-up with an ophthalmologist in 4-5 days (8).
Small orbital floor fractures are more likely to incarcerate orbital tissue. This may lead to compartment syndrome around the muscle, setting up an ischemic environment, which can cause muscular fibrosis (9). The longer the herniated tissue stays within the fracture, the greater the risk of damage to the tissue and subsequent residual motility deficits and diplopia. Jordan et al found that delayed release (2-3 weeks) lead to a slower recovery or only partial recovery (1). Furthermore, an observation period is less applicable in WEBOF patients because they have little or no sign of soft tissue trauma so a thorough clinical assessment is possible.
In summary, physicians should be aware of the signs, symptoms, and radiologic findings of orbital floor fractures. In addition, physicians should be aware of WEBOF as a subset of orbital floor fractures that may require more urgent surgical intervention.
Diagnosis: Orbital floor fracture with entrapment (white-eyed blowout fracture)
Epidemiology
|
Signs
|
Symptoms
|
Treatment
|
Rixen J, Call C, Carter KD. White-eyed blowout fracture. EyeRounds.org. January 11, 2012; Available from: https://eyerounds.org/cases/145-white-eyed-blowout-fracture.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links