
Chief Complaint: Blurred vision.
History of Present Illness: This patient is a 29-year-old white female who noticed that her vision had been getting progressively worse in the right eye (OD) over the past two weeks. She also felt that her central vision was diminished and she had pain with eye movements. The patient went to her local optometrist and was then referred to the University of Iowa for further evaluation.
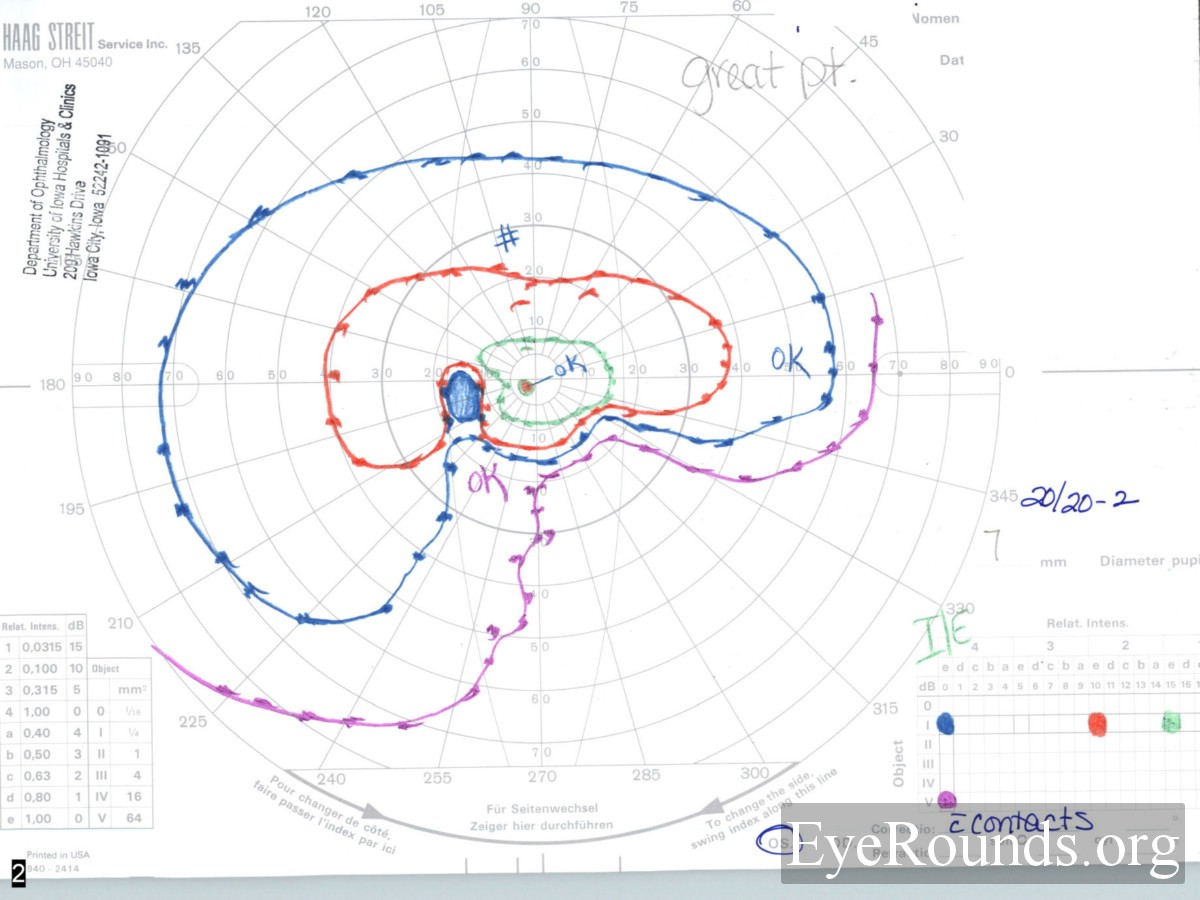
Past Ocular History: She had a similar episode four years prior to the current episode involving the left eye (OS). At that time she developed gradual onset blurred vision and pain with eye movements. She was seen by her local optometrist who diagnosed her with a swollen optic nerve. She was then referred to a neurologist who performed an MRI scan. The scan was reportedly normal and she was diagnosed with pseudotumor cerebri. She received no treatment and the vision slowly recovered over the next four months. However, she noted a persistent defect in her inferior nasal visual field OS.
Medical History: Three miscarriages at the end of the first trimester, otherwise unremarkable.
Medications: None.
Family History: No eye diseases, and otherwise noncontributory
Social History: Married, lives with her husband. No dietary restrictions. No exposure to cats.
 |
 |
 |
 |
 |
 |
 |
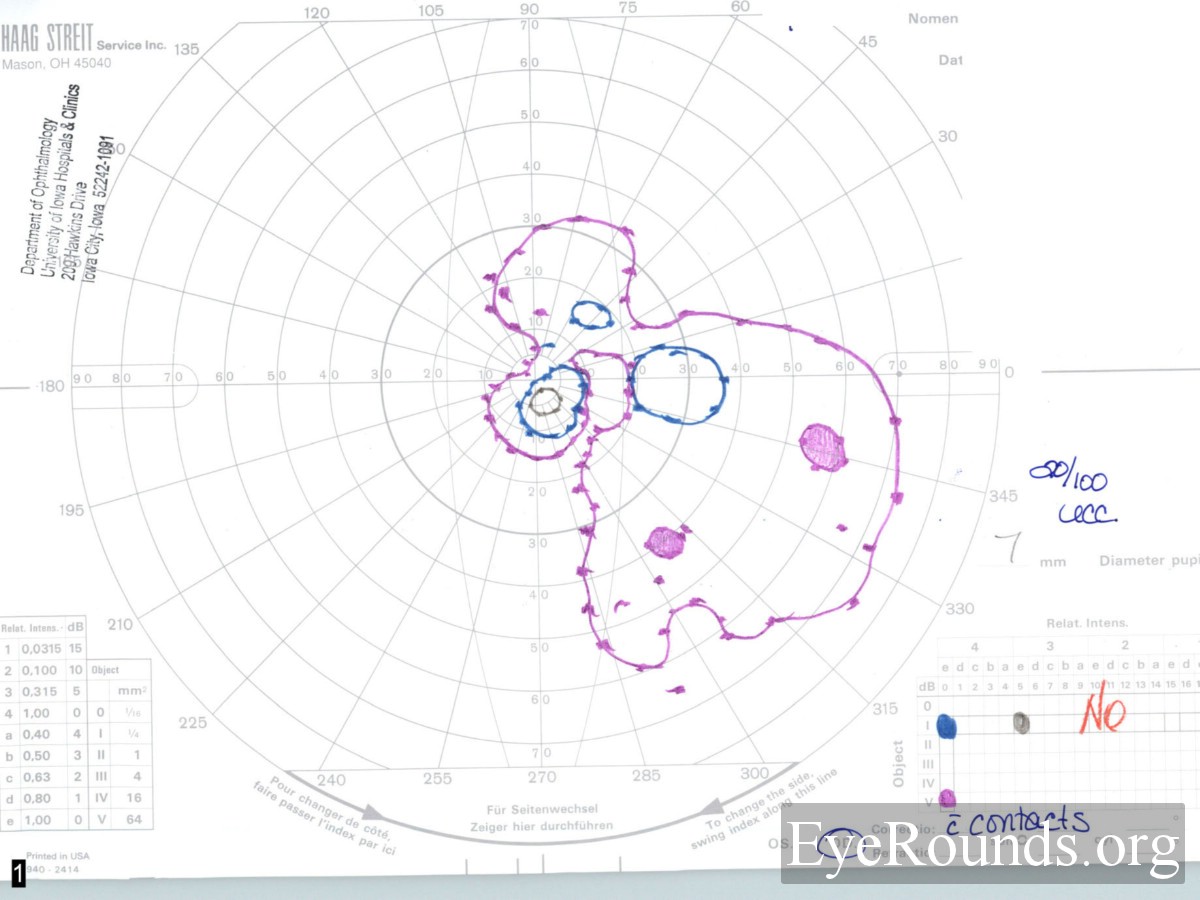 |
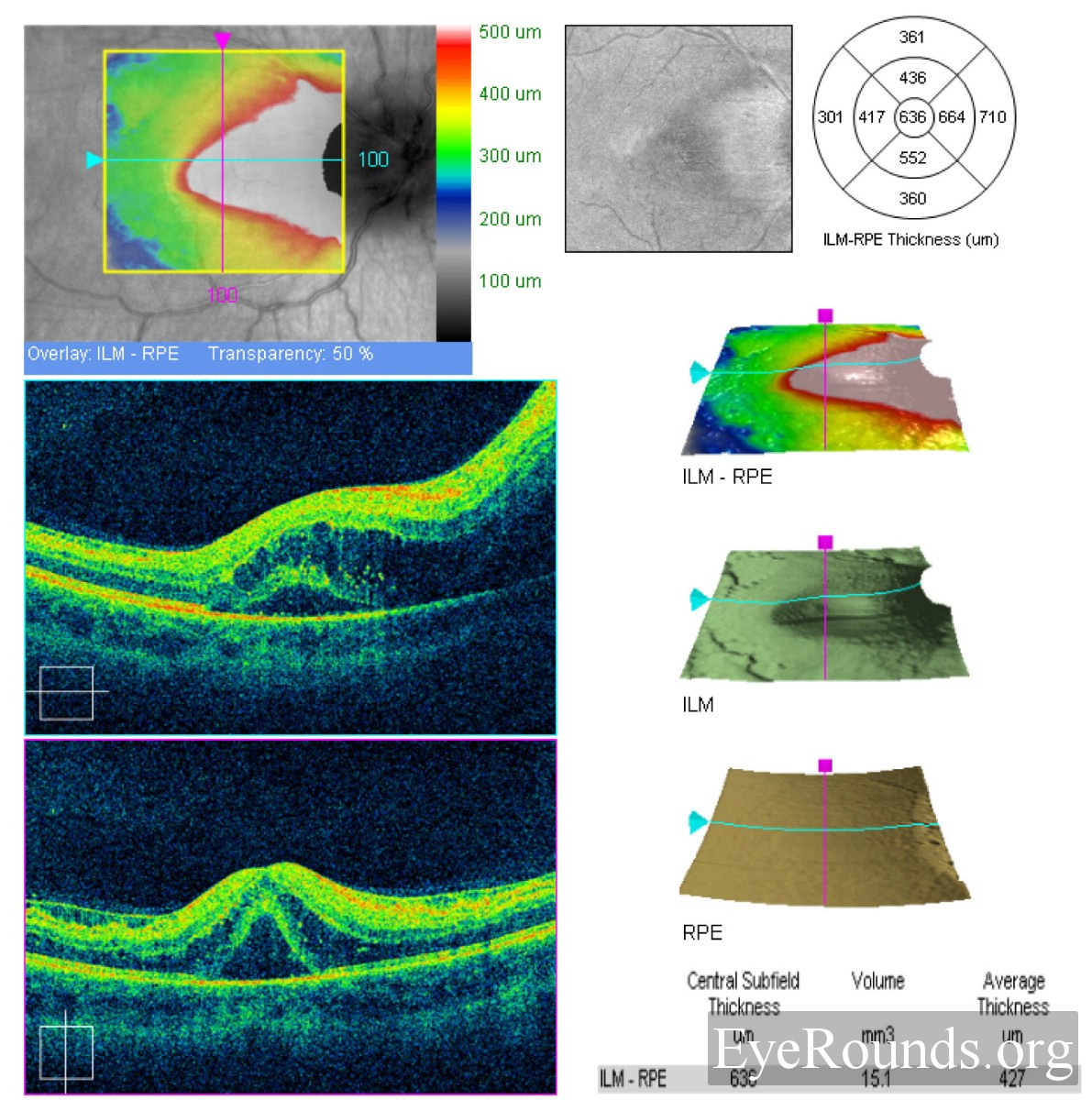
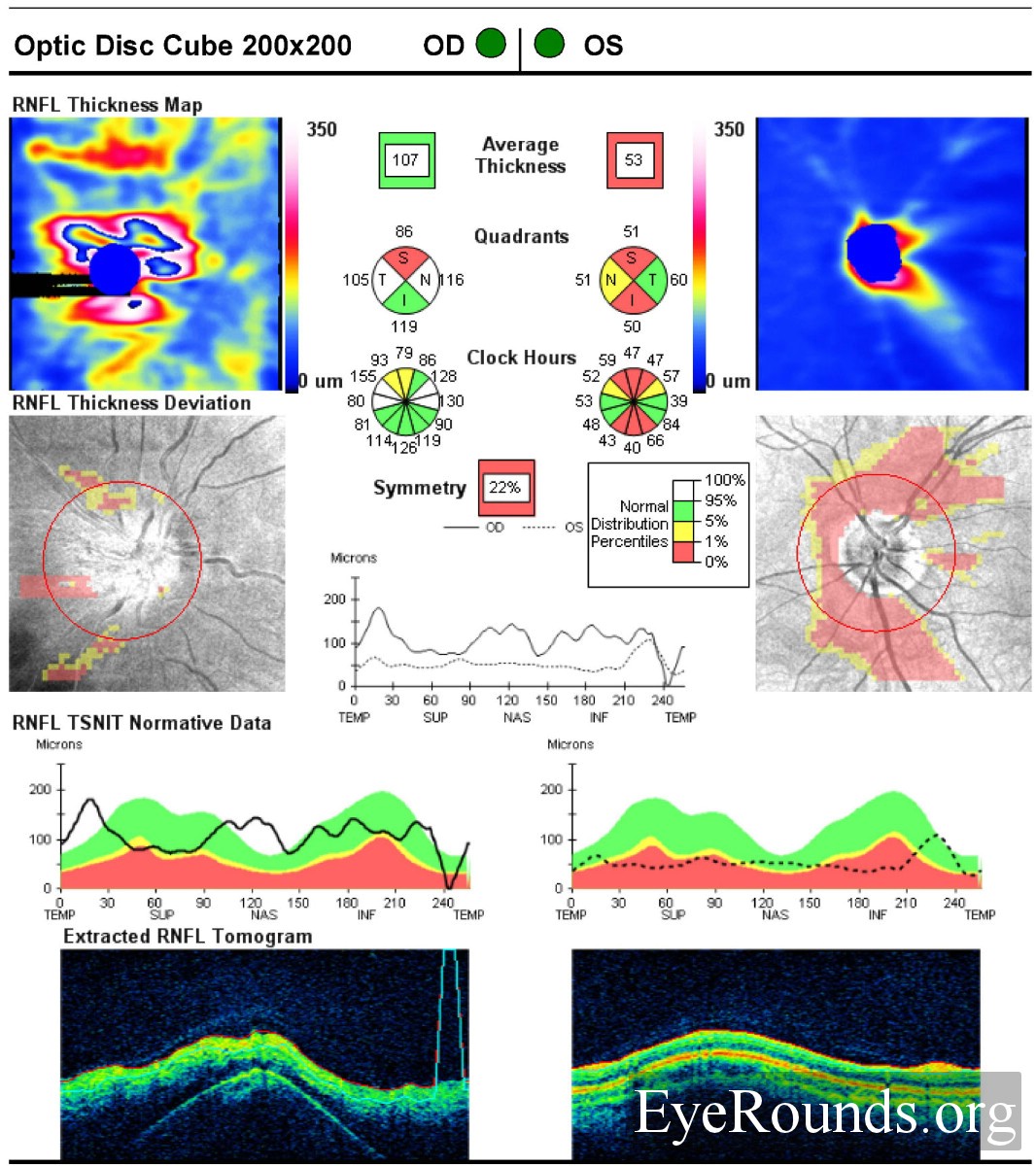
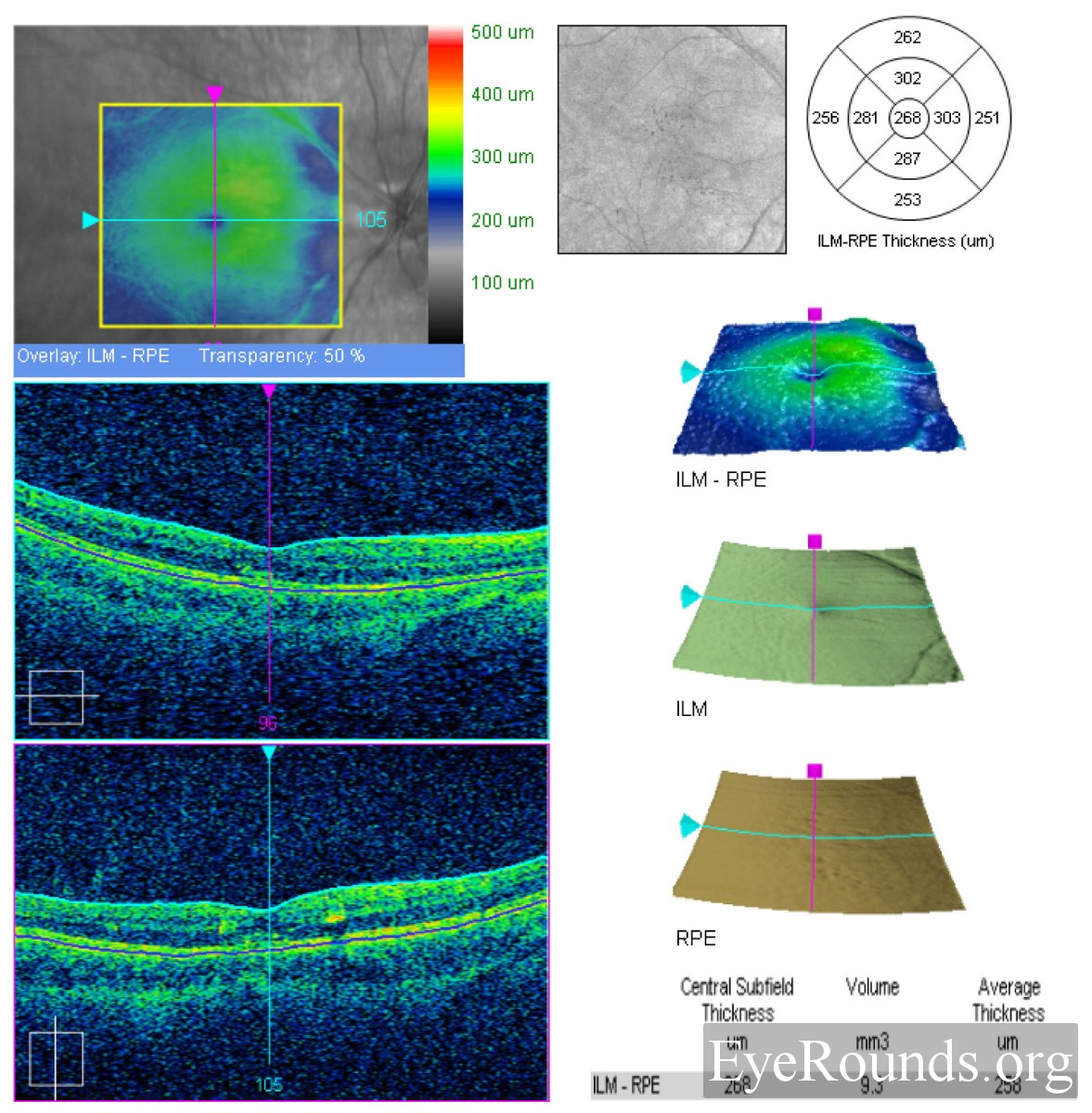
A presumptive diagnosis of neuroretinitis was made based on the patient's clinical appearance. Specifically, the appearance of the right optic nerve, the profound visual field loss as well as the accumulation of fluid in the outer plexiform layer are very suggestive of this condition. In addition, she had a history of a similar episode in the left eye associated with a swollen optic nerve years before. The appearance of optic atrophy and the inferior nasal scotoma in the left eye suggest that the previous episode also affected both the inner and outer retinal layers. However, the patient had very minimal if any exposure to cats. Therefore, a thorough work-up was performed to investigate other etiologies. Blood was drawn for testing of syphilis (RPR), antinuclear antigen (ANA), Bartonella Henselae, complete blood count (CBC), Lyme titers, and angiotensin converting enzyme (ACE). She was treated with a five day course of oral azithromycin and two weeks of oral prednisone and asked to return in one month.
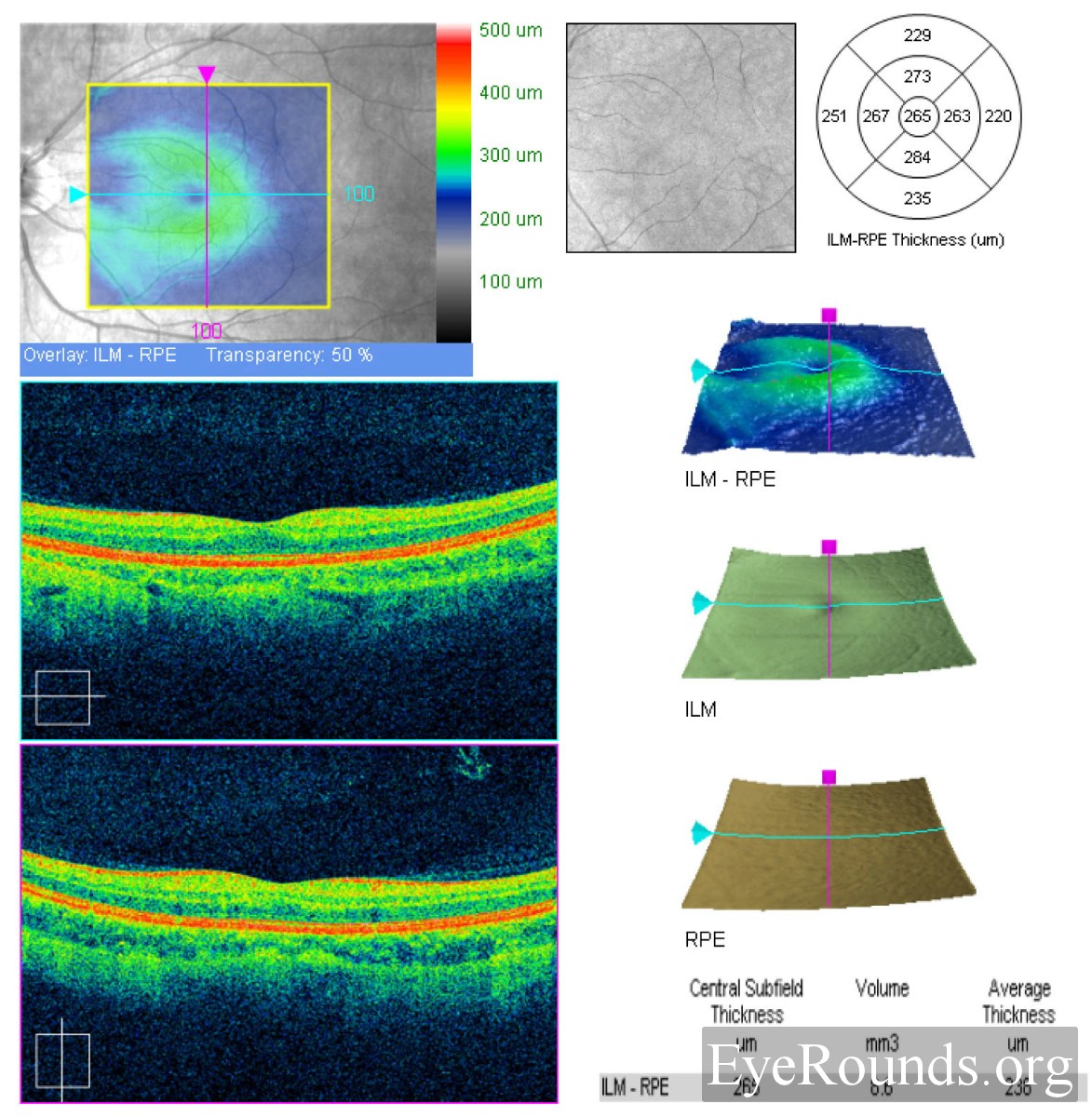
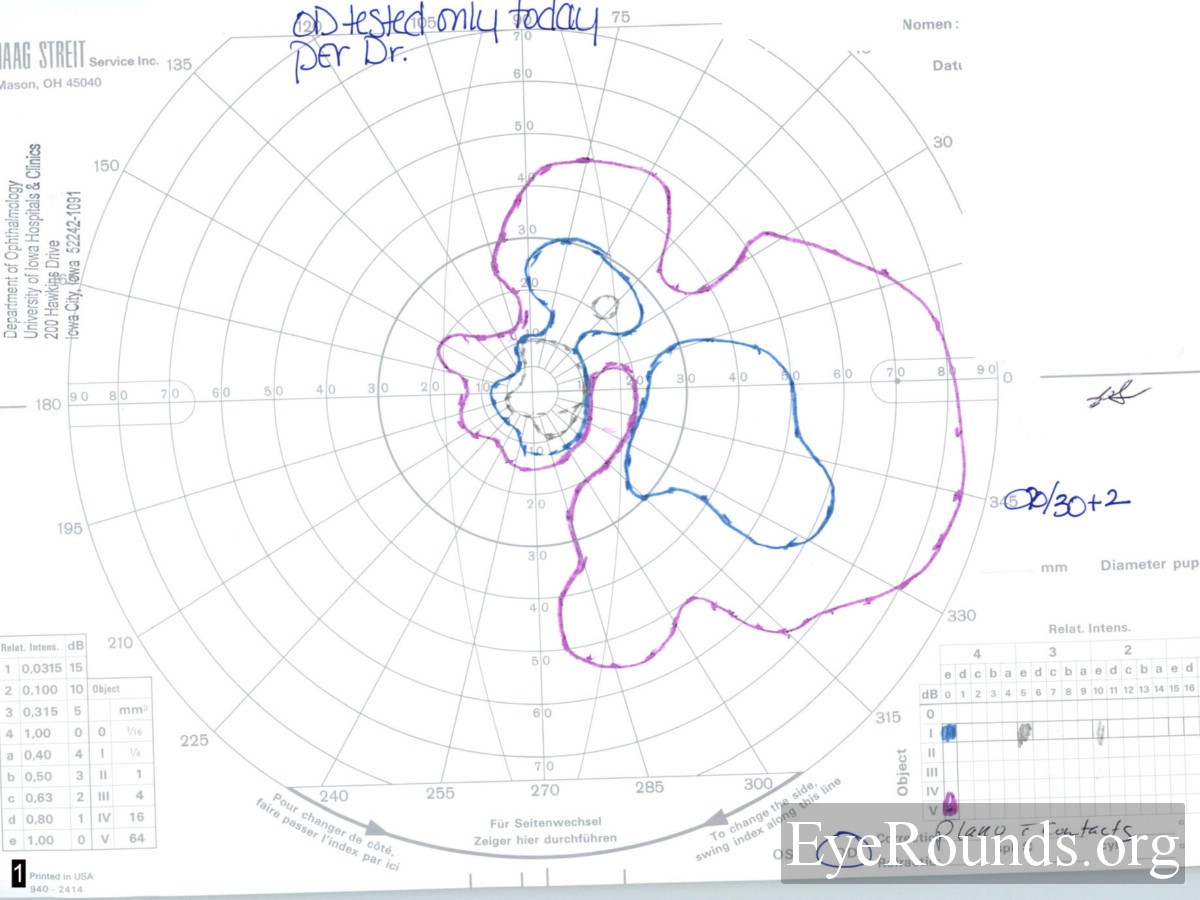
At here next appointment (one month later) she felt that her vision had improved to some extent in the right eye. Examination at that time revealed:
Laboratory work revealed negative testing for syphilis (RPR), Bartonella Henselae, and Lyme. The CBC, ANA, and ACE levels were all within normal limits. An MRI scan of the brain and orbits was performed on this date due to the atypical nature of the case. There was no mass, enhancing lesion, or demyelinating lesion seen on the scan. One month after this follow up visit, the patient developed symptoms of decreased vision in the left eye. She was not seen by a physician at this time and the symptoms resolved after about 2 weeks. She returned to the University of Iowa three months following her initial presentation and was felt to have suffered a recurrence of the disease in the left eye. Her visual acuity had decreased to 20/25 OS, there was mild disc edema, and her visual field was worse. She was offered treatment with systemic immunosuppressant medication but declined as she was actively trying to conceive a child.
 |
 |
 |
 |
Neuroretinitis is a clinical diagnosis made based on a constellation of ocular findings. These signs include unilateral painless visual loss, optic disc edema, macular edema, and the later development of a macular star. In the acute phase, vitreal cells are commonly seen. The majority of cases are thought to be due to current or previous infection with Bartonella henselae, a Gram-negative proteobacteria, however, infection with a number of different agents has been postulated to lead to the disease. Most patients with typical neuroretinitis generally suffer a single attack, with slow resolution of symptoms, with or without treatment. The visual prognosis is generally excellent.
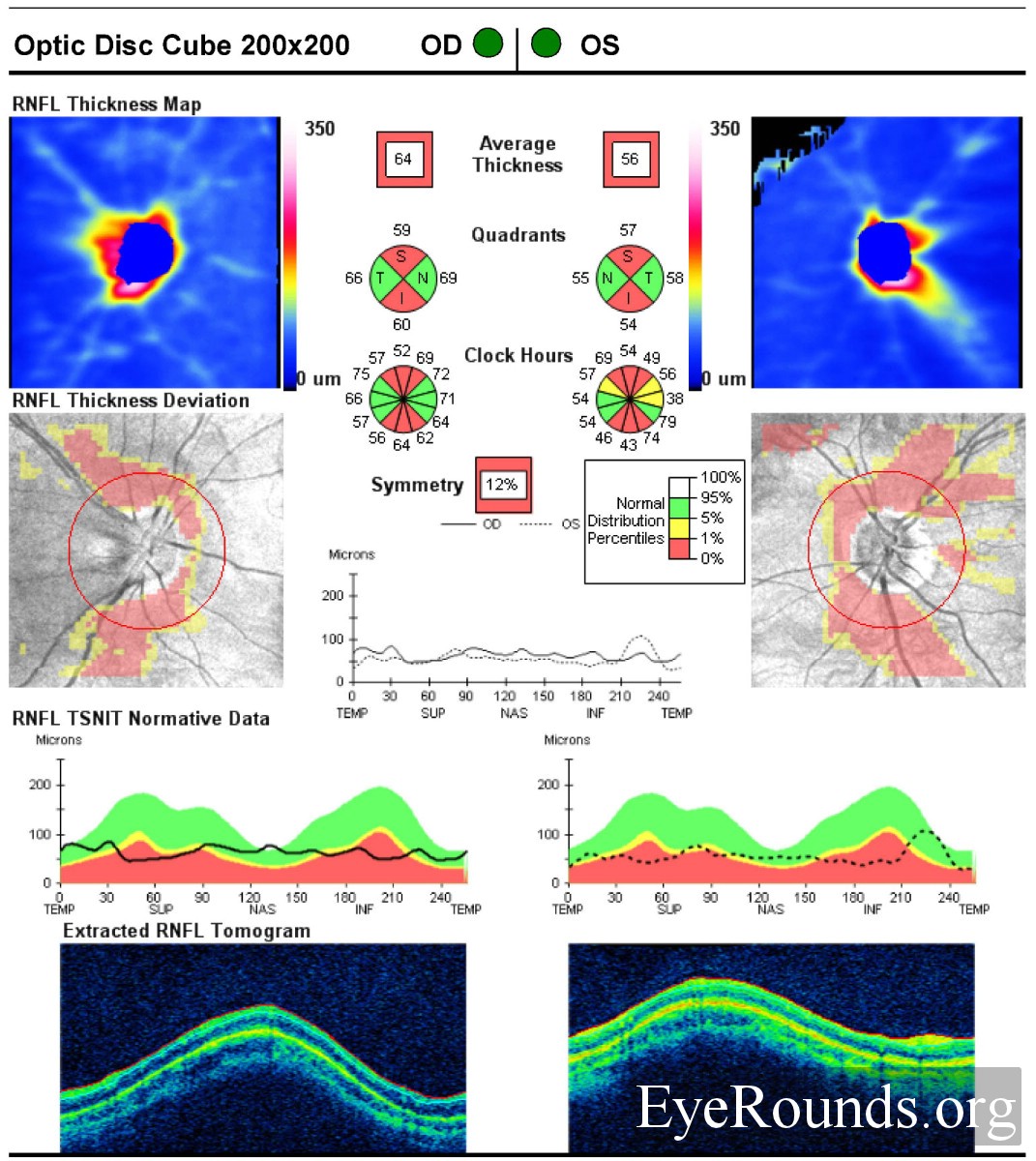
In contrast to the above stated clinical course, there exists a subset of patients who suffer repeated attacks of neuroretinitis involving the same or opposite eye. These patients, by definition, have negative serologic studies and thus the disease is referred to as idiopathic recurrent neuroretinitis. While this condition is uncommon, it can be visually devastating. Patients may develop permanent central or cecocentral scotomas, optic disc atrophy, and macular and retinal nerve fiber layer thinning. A number of case reports exists in the literature regarding this disease, its clinical course, and therapeutic options. In the current case, we decided to treat the patient with a short course of oral azithromycin to target Bartonella henselae as well as a short course of steroids to help decrease inflammation. This therapy was initiated upon our first clinical encounter with the patient, when the diagnosis of typical neuroretinitis was considered. However, as all of her serologic testing was negative, and she developed recurrent symptoms in the opposite eye, a diagnosis of idiopathic recurrent neuroretinitis was made. At that time we discussed the option with the patient of treatment with systemic immunosuppressive agents, but it was decided not to pursue this treatment, as she was trying to conceive.
To our knowledge, there has only been one case series reported in the literature of idiopathic recurrent neuroretinitis and potential treatment options. In their report, Purvin et al. describe a retrospective analysis of 30 patients with idiopathic recurrent neuroretinitis treated over a period of 18 years. Of these, seven patients were treated with ongoing immunosuppressive therapy which consisted of low dose oral prednisone and/or oral azathioprine. In each patient, treatment was initiated after several attacks of neuroretinitis which were generally treated acutely with a short course of oral steroids or antibiotics. At some point during their course, the patients began treatment with 50-150 mg/d of azathioprine and/or 10 mg/day of prednisone given on alternate days. Although their study was not designed as a prospective randomized study, the authors did find that treatment as described above decreased the rate of attacks per year by 72% (0.58 attacks per year prior to treatment versus 0.16 attacks per year after treatment).
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Cohen, AW, Kardon R. Recurrent neuroretinitis. EyeRounds.org. January 26, 2010; Available from: http://www.eyerounds.org/cases/107-Recurrent-Neuroretinitis.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
