Silent Sinus Syndrome:
36-year-old male with sunken left orbit (Enophthalmos)
Silent Sinus Syndrome:
36-year-old male with sunken left orbit (Enophthalmos)
Chief Complaint: 36-year-old male referred from Otolaryngology for a sunken left orbit.
History of Present Illness: A 36-year-old male was referred by his otolaryngologist to our oculoplastics clinic for evaluation of a sunken left orbit. This was noted while he was being evaluated for trouble breathing a few months prior. He has no complaints and has noticed no changes with his left eye.
Past Ocular History: Myopia
Medical History:
- Obstructive sleep apnea on nasal CPAP
- Obesity
- Deviated nasal septum
- Allergic rhinitis
Medications:
- Cetirizine 10mg 1 tab po daily
- Albuterol 90mcg Inhaler 2 puffs as needed for wheezes
- Fluticasone 50mcg nasal spray 2 sprays into each nostril daily
Allergies:
- Dust conjunctivitis
- Mold/Pollen Conjunctivitis and Rhinorrhea
Family History: Non contributory
Social History:
- Chews tobacco regularly
- Occasional alcohol
Review of Systems:
- 12 point review of systems negative aside from use of glasses for myopia and sinus congestion/allergic rhinitis
Ocular Exam:
- Visual Acuity. Chief Complaint: 20/15 OD, OS
- PUPILS: no RAPD OD, OS
- MOTILITY: Full OD, OS
- CONFRONTATIONAL VISUAL FIELD: Full OD, OS
- EXTERNAL: Normal OD, mild midfacial hypoplasia/enophthalmos OS
- Exophthalmometry: 19mm OD, 17mm OS
- Palpebral Fissure: 10mm OD, 8mm OS
- MRD1: 5mm OD, 4mm OS
- MRD2: 5mm OD, 4mm OS
- Levator function: 18mm OD, OS
- Lagophthalmos: 0mm OD, OS
- Lacrimal puncta: Normal UL/LL OD, OS
SLIT LAMP:
- Lids/Lashes: Normal OD, OS
- Conjunctiva/Sclera: Clear and quiet OD, OS
- Cornea: Clear OD, OS
- Anterior Chamber: Deep and Quiet OD, OS
- Iris: Normal architecture OD, OS
- Lens: Clear OD, OS
- Vitreous: Normal OD, OS
Dilated Fundus Exam:
- Disc: Normal OD, OS
- C/D Ratio: 0.3 OD, OS
- Macula, vasculature, and periphery: Normal OD, OS
Discussion:
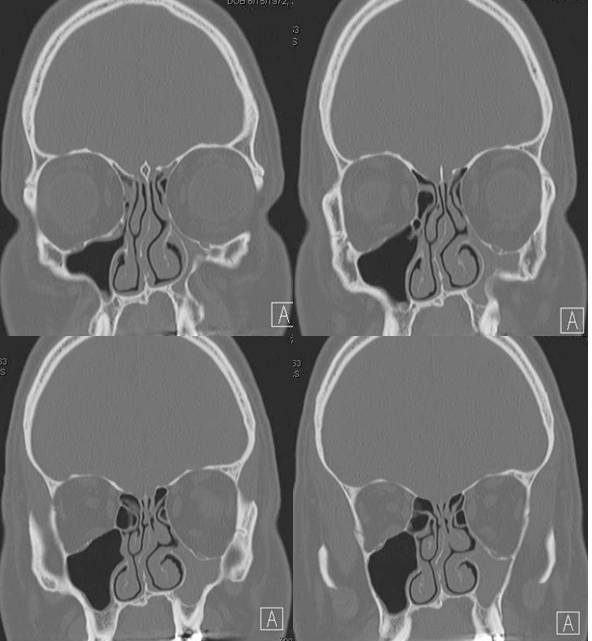
This patient initially presented to an otolaryngologist due to his worsening nasal obstruction even on CPAP and was thought to have sinus disease. A CT scan was performed and showed an opacified maxillary sinus with inward bowing of the bones of the maxilla, consistent with the diagnosis of silent sinus syndrome. The etiology and the pathophysiology of silent sinus syndrome is not clear but according to the available literature, the inciting cause is thought to be due to the hypoventilation of the maxillary sinus due to the obstruction of the osteomeatal complex. The hypoventilation over time results in resorption of gases into the capillaries of the sinus cavity, creating a negative pressure. Consequently, secretions accumulate which leads to chronic subclinical inflammation and atelectasis of the maxillary sinus. Biopsies, which may be performed to rule out malignancy if the suspicion is high, demonstrate respiratory epithelium with minimal lymphoplasmocytic infiltration and fibrosis. Bony fragments may show increased remodeling.
The differential diagnosis of enophthalmos is considerable (see below); however, it is imperative to rule out trauma-related orbital fractures in this young/middle aged population through extensive history taking as well as the physical exam and imaging.
According to the patient, he experienced no ophthalmologic complaints and was unable to recollect when these signs began. Analysis of all published cases thus far demonstrates that the mean duration of symptoms prior to presentation was 6.52 months.
The goal of treatment is to open the maxillary ostium with a wide enough antrostomy to prevent potential reobstruction. Orbital floor reconstruction can be done concurrently. Orbital floor reconstruction alone is not adequate and will not prevent recurrent enophthalmos in silent sinus syndrome.
Diagnosis: Silent Sinus Syndrome
EPIDEMIOLOGY
- Rare (approximately 84 reported cases between 1964 and 2004)
- Usually affects patients in the third to fifth decade
- No gender predilection
- First described in 1964
|
SIGNS
- Enophthalmos
- Hypoglobus
- Upper eyelid retraction
- Superior orbital sulcus deepening
- Fat loss in lower eyelid
- Malar depression
- Widening middle meatus
- Ipsilateral retraction of the middle turbinate toward the affected side
Imaging Signs: (most findings have been described on computed tomography)
- Fully developed, partially or completely opacified maxillary sinus
- Retraction of orbital floor leading to enophthalmos and increased orbital volume
- Orbital floor may be thinned or completely resorbed
- Occlusion of maxillary sinus infundibulum secondary to retraction of uncinate process
- Enlarged middle meatus
- Nasal septum deviation
|
SYMPTOMS
- Typically asymptomatic
- Spontaneous
- Fairly rapidly progressive but non progressive in the long term
- May report a sunken down appearance of the eye and/or deepening of upper eyelid sulcus
The following uncommon symptoms have also been reported:
- Diplopia
- Sinus complaints in the past
|
TREATMENT
Surgical 2-stage management
- Endoscopic maxillary antrostomy with or without uncinectomy by otolaryngologists
- Reconstruction of the orbital floor with placement of an implant such as a titanium-Medpor implant by oculoplastic surgeons
|
Differential Diagnoses of Secondary Enophthalmos:
- Silent Sinus syndrome
- Orbital fracture
- CSF shunting after childhood hydrocephalus
- Orbital varix
- Parry Romberg syndrome
- Linear scleroderma
- Chronic sinusitis
- Osteomyelitis
- Atrophy of orbital fat/contents (especially after surgery or trauma)
- Malignant infiltration
- Contraction of orbital fat (metastatic scirrhous carcinomas, most commonly breast)
- Anophthalmic enophthalmos
- Phthisis bulbi
- Pseudoenophthalmos
- Contralateral exophthalmos
- Horner's syndrome
References
- Gomez, J. et al, Enophthalmos in silent sinus syndrome. ENT Journal. 2008;9:496-498
- Illner, A. et al, The silent sinus syndrome: Clinical and radiographic findings. AJR Am J Roentgenol. 2002;178:503-506
- Nkenke, E. et al, Management of spontaneous enophthalmos due to silent sinus syndrome: a case report. Oral Maxillofac Surg. 2005;34:809-811
- Numa, WA. et al, Silent Sinus Syndrome: A Case Presentation and Comprehensive Review of All 84 Reported Cases. Ann Otol Rhinol Laryngol. 2005;114:688-694
- Rose, GE. et al, Clinical and radiologic characteristics of the imploding antrum, or silent sinus, syndrome. Ophthalmology. 2003;110:811-818
- Soparkar, CNS. et al, The silent sinus syndrome. A cause of spontaneous enophthalmos. Ophthalmology. 1994;101:772-778
- Thomas, RD. et al, Management of the orbital floor in silent sinus syndrome. Am J Rhinol. 2003;17:97-100
- Van Der Meer, JB. et al, The silent sinus syndrome: A case series and literature review. Laryngoscope. 2001;111:975-978
Suggested citation format:
Hong ES, Allen RC. Silent Sinus Syndrome: 36-year-old male with sunken left orbit (Enophthalmos). EyeRounds.org. January 4, 2010; Available from: http://www.EyeRounds.org/cases/102-Enophthalmos-Silent-Sinus-Syn.htm.
last updated: 01-04-2010
Image Permissions:

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.