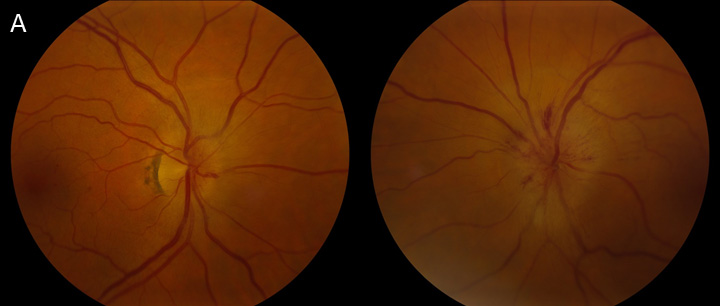
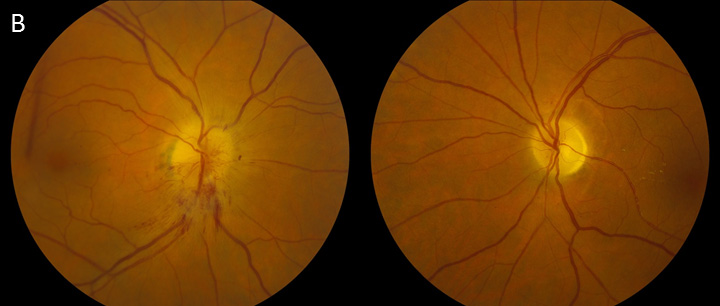
66-year-old morbidly obese hypertensive diabetic male with bilateral, sequential, acute painless vision loss from pseudo-Foster Kennedy syndrome. He initially presented with acute vision loss in the left eye and was noted to have disc edema with peripapillary hemorrhages OS and trace hyperemic disc edema OD (A) from non-arteritic ischemic optic neuropathy (NAION) OS and incipient NAION OD. Three months later, he developed acute painless vision loss OD. Dilated fundus examination at that time showed diffuse pallor OS and hyperemic sectoral disc edema OD (B). Of note, he had a normal MRI, denied symptoms of giant cell arteritis, and had normal inflammatory markers.
The presence of pallor in one eye and disc edema in the contralateral eye in the absence of an intracranial mass is called pseudo-Foster Kennedy syndrome. Our patient's presentation is consistent with bilateral sequential NAION, which is the most common cause of pseudo-Foster Kennedy syndrome. In cases of unilateral NAION, there is a 15% chance the contralateral eye will be affected within 5 years. True Foster Kennedy syndrome is the combination of papilledema in one eye and pallor in the other eye due to a large mass lesion causing compressive optic neuropathy and increasing intracranial pressure. True Foster Kennedy syndrome is very rare, and is typically caused by an olfactory groove meningioma.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links